1.
Anatomy of the stylohyoid apparatus:
The stylohyoid apparatus is formed by the styloid process,
the stylohyoid ligament and the lesser horn of the hyoid.
It is a complex structure of bone and ligament that connects the base of the skull with the body of the hyoid.
The first detailed description of it was made by Geoffroy Saint Hilarie in 1918,
according to Testut in his treatise on anatomy (Testut,
Latarjet 1977).
-Styloid process:
It is a thin and narrow protruberance of the temporal bone,
which originates in the lower part of the petrous portion,
immediately below the tympanic membrane.
Most authors cite an average length that ranges between 25 and 30 mm.
The styloid process descends in a caudal,
medial and anterior direction,
behind the pharyngeal wall in the area of the palatine fossa,
in the region known as the parapharyngeal or lateropharyngeal space,
between internal and external carotid arteries and very close to the glossopharyngeal nerve.
It presents an anterior angulation between 30 and 50º and a medial inclination between 10 and 27º.
Posterolaterally,
the styloid process is related to the facial nerve that emerges through the stylomastoid foramen and runs anteriorly and medially with respect to it; also with the hypoglossal nerve,
the occipital artery and the posterior belly of the digastric.
Medially it is related to the internal jugular vein,
the internal carotid artery and lingual,
facial,
superficial and maxillary temporal arteries and with accessory,
hypoglossal,
vague and glossopharyngeal nerves.
The glossopharyngeal nerve emerges from the jugular foramen and circulates below the styloid process,
very close also to the stylopharyngeus and stylohyoid muscles.
This position is the basis of the symptomatology of Eagle Syndrome.
In the styloid process originate the muscles that are part of the Riolan bouquet composed of the stylohyoid,
stiloglossal and stylopharyngeus muscles,
that play an important role during swallowing and chewing.
Along with this muscle group is inserted a ligamentous group,
formed by the stylohyoid and stylomandibular ligaments.
-Stylohyoid ligament:
It has been described as a fibrous cord of connective tissue with origin at the tip of the styloid process and insertion in the lesser horn of the hyoid.
It is medial with respect to the internal carotid and the hyoglossus muscle.
It is directly related to the posterior part of the medial surface of the submandibular gland.
Its possible calcification or mineralization is a controversial issue since both have been linked to the cause of elongation of the styloid process and therefore to the etiology of Eagle Syndrome.
-Lesser hyoid horn:
In the hyoid we can distinguish a body and four apophyses: two greater horns and two more cranial minor horns,
which are those that are part of the stylohyoid apparatus.
It serves as an insertion site for the stylohyoid ligament and the lower longitudinal and superior muscles of the tongue as well as the middle constrictor of the pharynx.
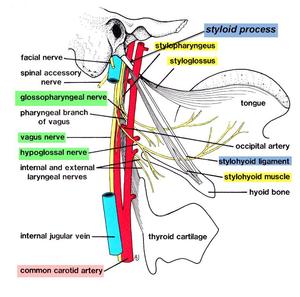
Fig. 1: Anatomy of the stylohyoid apparatus
References: free thesaurus
2.
Estilohyoid Apparatus and pathology:
2.1.
Etiology:
The etiology of the syndrome is still debated today.
When Eagle described the syndrome,
he thought that a surgical trauma or a chronic irritation could cause an osteitis,
a periostitis or a tendonitis of the stylohyoid complex,
producing a reactive ossifying hyperplasia of the styloid process.
In the etiology have traditionally been involved both an elongation of the styloid process above normal limits,
as a calcification or ossification of the stylohyoid ligament or even the stylomandibular ligament.
Other theories described are:
- Theory of abnormal angulation.
- Inflammatory theories ("tendinosis or insertion tendinitis").
- Fracture of the styloid process or the stylohyoid ligament,
especially if it is completely ossified from the tip of the apophysis to its insertion in the lesser hyoid horn.
- Formation of a possible pseudoarthrosis between the styloid process and the ossified fragments of the stylohyoid ligament.
- Rheumatic theory, secondary to a change in the direction of the process caused by the shortening of the cervical spine due to degenerative changes.
2.2.
Clinical types:
-Classic Eagle Syndrome:
Eagle syndrome is a rare entity,
first described by otolaryngologist W.
Eagle in 1937.
The symptoms would appear after a tonsillectomy and development of abundant scar tissue.
The etiopathogenic mechanism involved initially described by Eagle,
would be the entrapment of nerve endings of V,
VII,
IX and X cranial nerves in scar tissue,
although today it is thought that only the glossopharyngeal nerve would be affected.
The patient would present with mild and persistent pain in the pharynx,
typically located in the tonsillar fossa,
with irradiation to the homolateral ear.
Occasionally it would be accompanied by dysphagia,
odynophagia,
foreign body sensation in the pharynx and facial mild pain when moving the head.
It is common to palpate a mass in the tonsillar fossa that reproduces the symptomatology.
The radiograph showed an elongated styloid process and/or calcification of the stylohyoid ligament.
According to the original publication,
the anomaly is present in 4% of the population although they only present symptoms 4% of those affected,
especially if they are over 40 years.
-Stylocarotid artery syndrome:
Described by Eagle in 1949,
it would occur when the stylohyoid apparatus compresses and irritates the sympathetic plexus of the internal or external carotid artery.
In case of irritation of the perivascular plexus of the internal carotid,
cervical pain would occur when the head is turned or the neck compressed,
with irradiation to the supraorbital region,
vascularized area by the ophthalmic artery.
If the external carotid plexus is irritated,
the pain would refer to the infraorbital,
temporal,
auricular,
and occipital region.
The localization of pain in the neck when moving the head,
or irradiation to the eye is not common.
Dissection of the carotid artery caused by an elongated styloid process is a possible complication. The symptoms usually produce a sudden monocular blindness accompanied by pulsatile tinnitus and motor aphasia.
-Stylohyoid Syndrome:
According to Camarda,
there would be radiological evidence of an elongated styloid process and/or a calcified stylohyoid ligament but without a previous history of trauma or tonsillectomy.
It would consist of an early ossification,
in childhood or in adolescence that would manifest itself over the age of forty,
although there are cases described in children or teenagers.
It seems the most frequent clinical presentation,
since patients do not usually present a history of previous trauma or surgery.
-Pseudostylohyoid syndrome:
Described by Steinman in 1968,
in spite of the clinic there would be no radiological evidences neither of elongation nor of calcification of the ligament.
Neither would be associated traumatic,
or clinical signs of positive palpation.
The etiopathogenic mechanism involved would be an insertion tendonitis of the stylohyoid ligament,
or degenerative changes caused by age,
with the consequent loss of elasticity.

