I.
Clinical Presentation
Lisfranc injuries may present with varying degrees of swelling on the midfoot.
There are several clinical signs that could indicate a Lisfranc injury including midfoot pain while walking downstairs and pain upon palpation of the dorsal aspect of the tarsometatarsal joints.
Plantar ecchymosis has been considered pathognomonic for a Lisfranc injury and should initiate a rigorous evaluation.
II.
Conventional Radiography
Conventional radiography is the initial study on the evaluation of Lisfranc Injuries.
Images should be obtained in anteroposterior (AP),
lateral and 30°internal rotation oblique views 8.
On non-weight bearing radiographs the Fleck Sign,
a chip fracture at the surface of the base of M2 or C1,
is indicative of a Lisfranc fracture displacement representing an avulsion fracture from either of the Lisfranc ligament attachments 8,2.
The most common finding that indicates a Lisfranc injury is a malalignment or lateral step off at the 2nd tarsometatarsal joint caused by a lateral displacement of the base of M2 when compared to C2 8.
Other imaging findings that can indicate injury include: widening of >1mm between M1-M2 on AP radiograph,
disruption of the medial C2-M2 alignment line on the AP,
widening of >2mm between C1 and M2,
among others 2.
Nulley and vertullo recommended obtaining weight bearing radiographs whenever possible due to the fact that 50% of the low grade injuries appear normal on non-weight bearing images.

Fig. 3: Fractures of the base of the second, third and fourth metatarsals. There is lateral displacement of the second through fourth metatarsals as may be seen with Lisfranc's fracture/dislocation.
References: Department of Diagnostic Radiology, University of Puerto Rico

Fig. 4: Heavily comminuted fracture of the proximal first metatarsal bone involving the proximal metatarsal diaphysis and possibly the metatarsal base as well associated to a divergent Lisfranc fracture-dislocation.
References: Department of Diagnostic Radiology, University of Puerto Rico

Fig. 5: Comminuted displaced fracture of the base of the 2nd metatarsal and fourth metatarsal bones. Lateral displacement of the 2nd through 5th metatarsals. The is a comminuted minimally displaced intra-articular fracture of the medial cuneiform, anterior aspect cuboid bone and lateral cuneiform. Avulsion fracture of the middle cuneiform bone laterally.
References: Department of Diagnostic Radiology, University of Puerto Rico
III.
Computed Tomography (CT)
CT evaluation of a Lisfranc injury is helpful for evaluating the osseous anatomy,
articular alignment and aids in detecting subtle fractures that are commonly missed on conventional radiography.
CT provides a limited evaluation of the Lisfranc ligament complex whereas MRI provides detailed evaluation of soft tissue details.
CT plays an important role in evaluating the joint for pathologic widening.
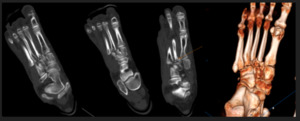
Fig. 6: Comminuted, displaced fracture of the second, third and fourth metatarsal bases. There is associated lateral displacement of the second, third and fourth metatarsal bones and the first metatarsophalangeal joint remains congruent, as can be seen with Lisfranc fracture/dislocation homolateral type.
References: Department of Diagnostic Radiology, University of Puerto Rico
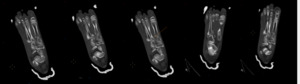
Fig. 7: Comminuted displaced fracture of the base of the 2nd metatarsal with associated lateral displacement of the 2nd through 5th metatarsals. Constellation of findings in favor of right foot Lisfranc fracture-dislocation.Additionally there are multiple fractures including minimally displaced chip fracture of the anterolateral dorsal corner of the middle cuneiform bone, comminuted minimally displaced fracture of the lateral cuneiform with fracture line extending to the cuneometatarsal and cuneocuboid joint and comminuted displaced fracture involving the anterior aspect cuboid bone, with fracture lines extending to the metatarsocuboid joint.
References: Department of Diagnostic Radiology, University of Puerto Rico
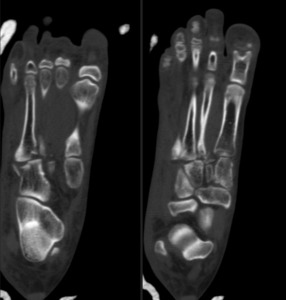
Fig. 8: Comminuted displaced fracture of the base of the 2nd metatarsal, as well as comminuted displaced fracture of the medial aspect of the base of the 4th metatarsal. Additionally, there is lateral displacement of the 2nd through 5th metatarsals. Additionally there are minimally displaced fractures of the medial cuneiform, middle cuneiform, lateral cuneiform and cuboid bone. Extensive right foot soft tissue swelling/edema. Constellation of findings in favor of right foot Lisfranc fracture-dislocation.
References: Department of Diagnostic Radiology, University of Puerto Rico
IV.
Magnetic Resonance (MRI)
MRI provides a detailed view of the Lisfranc ligament complex and is the ideal imaging modality for evaluating soft tissues when suspecting Lisfranc Injury.
The fluid sensitive sequences can detect bone marrow and soft tissue signal abnormalities that may indicate the presence of a Lisfranc injury.
The most common signs on MRI are: ligament tear,
ligament elongation and periligamentous edema 8.
Nulley and Vertullo proposed that low grade lisfranc injuries include isolated damage to the dorsal component or elongation of the interosseous parts of the Lisfranc ligament.
High impact injuries affect the plantar component of the ligament.
MRI is helpful in depicting injuries to other ligaments that contribute to midfoot stability.
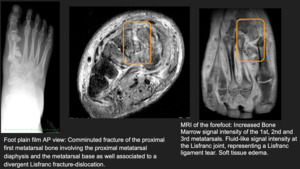
Fig. 9
References: Department of Diagnostic Radiology, University of Puerto Rico
