I. Introduction
The Lisfranc joint complex is an essential component for midfoot and forefoot stability.
Lisfranc injuries can be classified depending on the etiology of the injury.
High impact injuries,
also called Lisfranc Fracture-Displacement,
occur as a result of motor vehicle trauma and carry a high morbidity.
Low impact injuries,
also called Lisfranc Injuries or Midfoot Sprains,
are common among athletes.
A significant amount of Lisfranc injuries (35%) are initially missed due to soft tissue swelling or being overlooked due to multiple injuries.
A delay on the diagnosis increases the risk for midfoot instability,
deformity and debilitating osteoarthritis.
Missed Lisfranc ligament injuries are among the most common cause of litigation against radiologist and emergency physicians 8.
It is important to understand the anatomy and injury pattern to be able to diagnose lisfranc injuries.
II.
Anatomy
The Lisfranc joint complex is composed of nine bones: the five metatarsals (M),
the three cuneiforms (C),
and the cuboid (Cu).
The second metatarsal is the key component of the Lisfranc joint complex,
it articulates between C1 and C3 forming a mortise and tenon joint.
It has been described that the longer the medial mortise depth it allows for a broader and stronger lisfranc ligament which protects against injury 2.
There are three synovial articulations that divide the midfoot into three columns.
The lateral column,
encompasses the articulation between M4,M5 and the Cuboid,
it is the most mobile column and is protected against post-traumatic instability.
The middle column is composed of M2,M3 and C2,C3; the medial column is composed of the articulation between C1 and M1.
The middle and medial columns are more rigid than the lateral column.
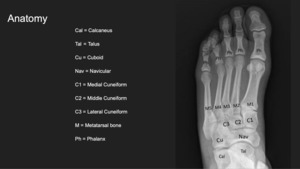
Fig. 1: Tarsal and metatarsal anatomy.
References: Department of Diagnostic Radiology, University of Puerto Rico
The lisfranc ligament is composed of three segments:
1- Lisfranc ligament proper: the interosseous ligament between C1-M2
2- Dorsal Lisfranc ligament: the connection of the dorsal aspect of C1 and M2.
The dorsal Lisfranc ligament is the weakest part,
explaining why most injuries result with a dorsal displacement.
3- Plantar Lisfranc ligament: the connection between the plantar aspect of C1 and M2,M3.
The plantar and interosseous ligaments are the strongest attachments; injury to them results in transverse midfoot instability and widening of the C1-M2 joint 8.
Three intermetatarsal ligaments exist between M2-M3,
M3-M4,
M4-M5.
There is no intermetatarsal ligament joining the M1-M2 bones causing a point of weakness in which the Lisfranc ligaments are responsible for its stability.
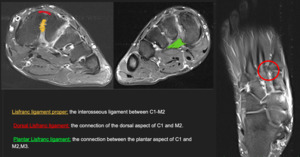
Fig. 2: Lisfranc Ligament Anatomy.
References: Department of Diagnostic Radiology, University of Puerto Rico
III.
Mechanism of Injury
A.
High Impact Injuries are the result of direct forces applied to the TMT joint for example crush injuries or motor vehicle accidents.
This type of injury often results in multiple injuries which may hinder the radiologic evaluation.
The displacement of the metatarsals depends on the the direction of the force of injury which can result in plantar or dorsal displacement.
B.
Low Impact Injuries are the result of indirect forces leading to a dorsal displacement of the metatarsals.
There are two mechanisms of injury that result in low impact injuries:
1- Forefoot Abduction: occurs when the hindfoot is fixed and the forefoot is suddenly abducted resulting in a dorsal displacement of the metatarsals.
This type of injury is common among surfing and equestrian sports 7.
2- Forced Plantar Flexion: occurs when there is an axial force applied to a foot in plantar flexion where the toes are dorsiflexed at the metatarsophalangeal joint 7.
This type of injury is common among ballerinas,
football players,
gymnasts,
among others 8.
IV.
Classification Systems:
A.
Quenu and Kuss: their classification system relies on the position of the metatarsal bones without regarding the mechanism of injury 8.
1- Homolateral: is the most common pattern and involves the displacement of all 5 metatarsals in the same direction.
2- Isolated: is the least common and involves the displacement of only a few metatarsals.
3- Divergent: occurs when the first metatarsal is displaced medially and the other metatarsals are displaced laterally.
B.
Myerson classifies the injuries depending if they demonstrate a complete (all joints) or partial (some joints) incongruity at the tarsometatarsal joints.
Type A: there is complete incongruity and all five metatarsals are displaced in the same direction.
Type B: there is partial incongruity which is limited to a particular column.
Type B can be further subdivided into: B1,
partial,
in which there is medial displacement of M1; B2 lateral displacement any of the M2-M5.
Type C: there is a divergent displacement in which metatarsals are displaced in different directions.
Type C can be further classified into C1,
partial,
in which M1 and some of the metatarsals are displaced on opposite directions.
Type C2,
complete,
M1 is displaced on an opposite direction to all of the other metatarsals.
C.
Nulley and Vertullo proposed a classification system which included the low grade injuries.
They proposed a mechanism of injury that initially involve the dorsal aspect of the Lisfranc joint complex,
followed by interosseous ligaments and subsequent involvement of the plantar ligaments.
Stage 1: Refers to a low grade sprain of Lisfranc Ligament Complex.
there is a dorsal capsular tear but the joint remains stable.
On imaging there is no displacement or loss of arch height.
Stage 2: On imaging there is a 2-5mm diastasis between C1 and M2 but no loss of arch height on the lateral radiographs.
Stage 3: On imaging there is a more than 5mm diastasis between C1 and M2 and a loss of arch height which is indicated by a decrease in the distance between the plantar aspect of M5 and C1 on lateral radiographs.
