- In this work,
we outline the important pathophysiologic characteristics of primary neoplasms of the small intestine including their changing epidemiology,
risk factors for development,
and relative frequency in each individual small intestine segment.
- Multiphase CT is the protocol of choice for the detection of many of these neoplasms,
because some tumors are best visualized in the arterial phase and others in portal phase.
- We review the wide range of malignant and benign small bowel tumors and tumor-like lesions including carcinoid,
adenocarcinoma,
lymphoma,
gastrointestinal stromal tumors,
lipomas,
adenomas.
1- Benign tumors
*Leiomyomas (Fig. 1 )
- These originate in the circular or longitudinal muscle layers and rarely in the muscularis mucosa.
- Four types have been identified depending on their pattern of growth: intramural,
intraluminal (or submucosal) that is the most common,
extraluminal (or subserosal) and bidirectional (or dumbbell-shaped).
- Usually they are asymptomatic,
but they can cause intraluminal bleeding when they are seat of necrosis and ulceration.
- The jejunum is the most frequent location of leiomyomas,
followed by the ileum and the duodenum,
although they are rare in the small intestine.
- On CT,
leiomyomas typically appear as sharply defined spherical or ovoid masses ranging from 1 to 10 cm.
They display homogeneous soft-tissue density and uniform contrast medium enhancement.
Calcifications can occasionally be present.
It can be difficult to distinguish benign from malignant leiomyomas based on imaging alone.
Marked contrast enhancement in the absence of metastases or mesenteric changes is compatible with benign leiomyomas.
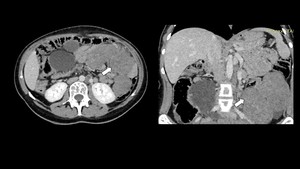
Fig. 1: Axial and coronal enhanced abdominal CT showing multiple leiomyomas of the jejunm (arrows).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
*Adenomas ( Fig. 2 ) :
- Adenomas are the most common benign small bowel tumors,
accounting for 14- 20% and consisting of glandular epithelium.
- They can be divided in two main histologic groups: villous and tubular adenomas. Villous adenomas have a higher potential for malignant transformation than tubular adenomas.
The adenoma-carcinoma sequence is comparable to their counterpart in the colon and it has been estimated that approximately one-third of solitary small bowel adenomas will transform into invasive carcinomas.
Polyposis syndromes are a significant risk factor and should be suspected when multiple lesions are observed.
Additionally,
patients with a sporadic duodenal adenoma should be screened for colorectal cancer because of an increased risk of colorectal neoplasia.
- Small bowel adenomas can be clinically silent or cause bleeding,
obstruction,
jaundice (if they involve the ampulla of Vater) and intussusception .
On CT, they appear as a sessile or pedunculated well-defined,
soft tissue mass surrounded by a thin rim of oral contrast showing moderate enhancement after intravenous contrast administration.
MPR (Multiplanar reconstruction) images can help to differentiate adenomas from adenocarcinomas by identifying smooth margins,
lack of mesenteric invasion and clear fat planes around the tumor.
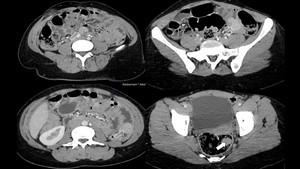
Fig. 2: Peutz–Jeghers syndrome in a 30-year-old woman with abdominal pain. Axial enhanced abdominal CT scan show multiple intraluminal enhancing polyps of the jejunumm, the ileum (empty arrow)and the rectum(white arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
*Lipomas ( Fig. 3 ,
Fig. 4 ) :
- Lipomas are the second most common benign tumors of the small bowel and consist ina well-circumscribed proliferation of adipocytes.
They are mostly solitary,
may grow to a large size and can undergo necrosis,
cystic degeneration or calcification.
- Although most of cases small bowel lipomas are asymptomatic,
clinical manifestations can include intestinal bleeding due to ulceration or incomplete small bowel obstruction episodes due to intussusception.
On both CT and MRI,
lipomas are usually easy to diagnose on account of their density (-80 to -120 HU) or their intensity following that of fat on all sequences.
- Lipomas are usually entirely of fat density without solid components.
If a solid non-fat component is seen then the possibility of the mass representing a liposarcoma should be entertained,
although these are exceedingly rare.Overlying ulceration may result in some non-fat density/intensity stranding near the mucosal surface.
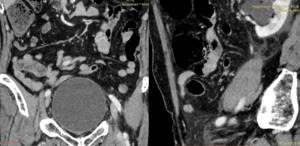
Fig. 3: Lipoma in a 60-year-old woman.
coronal and sagittal contrast-enhanced CT scan show a fatty mass in the jejunum (empty arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
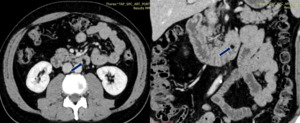
Fig. 4: Lipoma in a 40-year-old woman. Contrast-enhanced axial and coronal CT scans show a fatty mass (arrow) in the duodenum.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
2- Malignant tumors :
*Adenocarcinomas
- Adenocarcinomas are the second most common type of small bowel malignancy,
and account for approximately 30-40% of primary neoplasms. The vast majority of these are located at the duodeno-jejunal junction with incidence decreasing distally to this.
- Adenocarcinomas typically arise from glandular epithelium composed of tubular or villous structures.
- CT features of small bowel adenocarcinoma may appear as a solitary soft-tissue mass with annular or eccentric luminal narrowing .
They can also appear as a discrete tumor mass or ulcerated lesion,
usually involving a short segment and may cause partial or complete bowel obstruction.
CT typically demonstrates heterogeneous attenuation and moderate enhancement.
CT is useful modality for the detection of the primary lesion,
locating the transition point in a case of acute intestinal obstruction due to the intraluminal mass or an intussusception and for demonstrating local lymphadenopathy and distant metastases.
*Gastro intestinal stromal tumors(GIST):
- These are the most common mesenchymal tumors of the gastrointestinal tract originating in the interstitial cell of Cajal (an intestinal pace-maker cell in normal myenteric plexus) and characterized by mutations in the KIT gene.
- Also known as Gastrointestinal Stromal Tumours (GISTs),
these tumours account for 15-20% of all primary small bowel malignancy. There is a spectrum of disease,
and only around 20% of all GISTs are malignant. Distribution is spread across the whole small bowel,
in contrast to carcinoid and adenocarcinoma. Neurofibromatosis type 1 is a large risk factor for the development of multiple,
small GISTs.
- GISTs may be intraluminal,
submucosal or subserosal in location and appear as smooth,
well-defined masses.
- The CT features of GISTs vary greatly,
depending on the size and aggressiveness of the tumor and the time of presentation during the course of the disease.
Primary GISTs are typically large,
hypervascular,
enhancing masses on contrast-enhanced CT scans and are often heterogeneous because of necrosis,
hemorrhage,
or cystic degeneration at the time of presentation .
Ulceration and fistulization to the gastrointestinal lumen are also common features of GISTs .
Often,
tumor vessels can be seen within the tumors .
The masses usually displace adjacent organs and vessels,
but direct invasion of the adjacent structures is sometimes seen with advanced disease .
It can be difficult to identify the origin of the mass because of its large size and prominent extraluminal location.
Bowel obstruction is rare.
*Carcinoid tumors ( Fig. 5 ,
Fig. 6 ,
Fig. 7 )
- The group of neuroendocrine tumours are the most common form of primary small bowel neoplasm and account for 35-42% of all small bowel malignancies.
- Most of these slow-growing tumours occur in the distal ileum,
followed by the jejunum. Primary involvement of the duodenum is rare – up to 2% of cases.
Up to 35% of carcinoid tumours also have multiple primary sites.
- They are well differentiated neuroendocrine tumors,
arising from argentaffin cells.
- The typical carcinoid syndrome usually arises when the carcinoid tumors have metastasized to the liver,
meaning that the secretory products of these tumors gain direct access to the systemic circulation avoiding the liver’s metabolism.
- Symptoms are characterized by flushing,
diarrhea,
abdominal pain,
bronchospasm and rarely with pruritus due to histamine excess.
- Carcinoids < 1 cm rarely metastasis,
while lesions > 2 cm have 30 % risk of lymph node metastases.
Carcinoids vary in appearance from small submucosal lesions to large ulcerating masses.
It can be difficult to differentiate primary carcinoid tumors from other lesions of the small bowel; however,
the desmoplastic reaction produced by these tumors is characteristic.
- A soft-tissue mass with calcification,
desmoplastic reaction,
and avid contrast enhancement is almost pathognomonic for carcinoids.
Lymphadenopathy and metastases to the liver,
to omentum and ascites may be demonstrated.
Small bowel obstruction secondary to the desmoplastic reaction or serosal disease is a recognized complication.
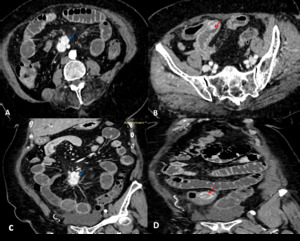
Fig. 5: Axial and coronal enhanced abdominal CT scan show small bowel neuroendocrine tumor(red arrow)with mesenteric localization(blue arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
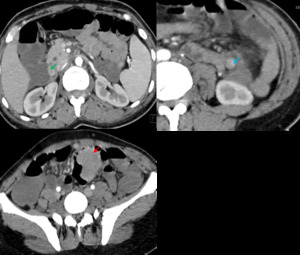
Fig. 6: Axial enhanced CT scan show three masses developed at the expense of an ileal loop (red arroow) , a jejunal loop (blue arrow) and the third portion of the duodenum(green arrow)related to a neuroendocrine tumor.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
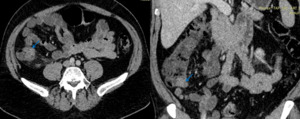
Fig. 7: Axial and coronal enhanced abdominal CT scan show carcinoid tumor of the base of the appendix (blue arrow).
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
*Lymphoma ( Fig. 8 )
- Approximately 15-20% of all primary small bowel malignancy is lymphomatous in nature.
Most of these are non-Hodgkin B-cell type disease,
accounting for approximately 40% of tumours. Other histological types are seen less commonly,
including Burkitt’s,
follicular and T-cell lymphomas. Risk factors include HIV,
immunosuppression,
coeliac disease and inflammatory bowel disease. Small bowel lymphomas are most commonly found in the ileum.
- These tumors are characterized by a vague clinical presentation of abdominal pain,
anorexia,
and weight loss.
- The spectrum of radiological presentations of small bowel lymphoma includes a circumferential or cavitatory mass,
aneurismal dilatation of the bowel,
mesenteric nodal disease with secondary small bowel involvement and polypoidal disease.
Dilatation of the bowel lumen is characteristic of intestinal involvement and is recognized as a central or eccentric collection of gas or contrast within a usually ulcerated mass .
Mural infiltration presents as intestinal wall thickening,
nodular or concentric,
and appears relatively homogeneous in density showing a moderate peripheral enhancement after intravenous contrast administration.
Mesenteric involvement is frequently present.
It may appear as bulky mesenteric or retroperitoneal adenopathy or ill-defined confluent mesenteric masses encasing loops of intestine.
Ulceration,
necrosis and fistulous tracts to adjacent bowel loops are also clearly demonstrated.
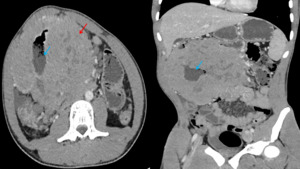
Fig. 8: Axial and coronal enhanced CT showing intraperitoneal mass(red arrow)centered on a jejunal loop(blue arrow) providing necrosis areas responsible for dilatation of jejunal loops upstream related with a lymphoma.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia
*Secondary tumors :
- Secondary neoplastic involvement of the small bowel is more frequent than primary small intestinal neoplasia.
Extrinsic tumors involve the gut by hematogenos metastases,
by direct invasion or by intraperitoneal seeding.
- CT will demonstrate extension of disease directly to the small bowel from an adjacent primary malignancy in addition to any complication such as bowel or biliary obstruction.
- Haematogenous spread is common with breast,
lung,
renal cell and melanoma malignancies,
while intraperitoneal seeding is often seen with mucinous ovary,
appendix and colonic neoplasms.

. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
and the rectum(white arrow). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
 in the duodenum. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
with mesenteric localization(blue arrow). References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
 , a jejunal loop (blue arrow) and the third portion of the duodenum(green arrow)related to a neuroendocrine tumor.
References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")
centered on a jejunal loop(blue arrow) providing necrosis areas responsible for dilatation of jejunal loops upstream related with a lymphoma. References: Department of radiology, Charles Nicolle Hospital , Tunis, Tunisia")