ECR 2019 / C-3185
Urological urgencies. What the urólogo need to know
Congress:
ECR 2019
Poster Number:
C-3185
Type:
Educational Exhibit
Keywords:
Urinary Tract / Bladder, Emergency, Abdomen, CT-High Resolution, Ultrasound, Ultrasound-Colour Doppler, Surgery, Acute, Infection, Trauma
Authors:
Z. FIGUEROA MARQUEZ 1, G. A. Averanga Ticona2, G. G. Leal2, Y. P. Narváez Rojas2, J. Crosta2, F. A. Abramzon2; 1pablo nogues/AR, 2Buenos Aires/AR
DOI:
10.26044/ecr2019/C-3185

Fig. 2:
RENAL CALCULI. Hyperechogenic image that generates posterior acoustic shadow.

Fig. 3:
RENAL CALCULI. Hyperechogenic foci with acoustic shadowing.

Fig. 4:
STAGHORN CALCULUS, also called coral calculi, are renal calculi that obtain...

Fig. 5:
STAGHORN CALCULUS
, which gives the appearance of turbulent blood flow.")
Fig. 6:
TWINKLING ARTIFACT is an artifact seen with Color Doppler that is the result of...

Fig. 8:
HYDRONEPHROSIS. Dilatation of the renal pelvis and proximal ureter.

Fig. 9:
HYDRONEPHROSIS:
Sine-parenchyma ratio thinned. Dilatation of calices and renal...

Fig. 10:
PYELOCALICIAL DILATATION: hydronephrosis associated with ureteral dilation.

Fig. 11:
Marked hydronephrosis with thinning of the cortex

Fig. 12:
BLOOD MOLD

Fig. 13:
PYELONEPHRITIS:
Poorly defined hypoechoic parenchymal areas as signs of...

Fig. 14:
PYELONEPHRITIS:
Hypoechoic areas as signs of edema.
Loss of...

Fig. 15:
PYELONEPHRITIS. Increased in the color Doppler signal as inflammatory signs.

Fig. 16:
RENAL ABSCESS. Well-defined hipoechoic area within the cortex.

Fig. 17:
RENAL ABSCESS. Hypodense area, with ring enhancement after contrast.

Fig. 18:
FOURNIER GANGRENE.
a. y b. Echogenic gas foci in cavernous bodies of the...

Fig. 19:
FOURNIER GANGRENE: Subcutaneous emphysema is visualized

Fig. 20:
ORCHYEPIDIDIMITIS
a. Epididymal head enlarged with increased...

Fig. 21:
ORCHITIS.
Increase in vascularization in the left testicle coinciding with...

Fig. 22:
TESTICULAR TORSION.
Left testicle enlarged, hypoechoic, without...
.
d. Discontinuity in the tunica albuginea (thick arrow).")
Fig. 23:
TRAUMA TESTICULAR:
a. Testicle with a not well defined lesion, heterogeneous,...

Fig. 24:
TESTICULAR TRAUMA.
Testicular heterogeneous parenchyma with loss of the...
 associated with a hematoma in the corpus cavernosum.")
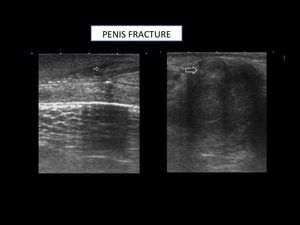
Fig. 25:
PENILE FRACTURE: Rupture of tunica albuginea (arrow) associated with a hematoma...

Fig. 26:
WUNDERLICH SYNDROME.

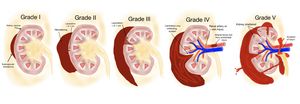
Fig. 27:
GRADING SCALE OF KIDNEY INJURIES

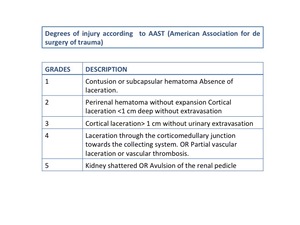
Fig. 28:
DEGREES OF INJURY ACCORDING TO AAST

Fig. 29:
GRADE I: Contusion or subcapsular hematoma Absence of laceration

Fig. 30:
GRADE III: Cortical laceration> 1 cm without urinary extravasation

Fig. 31:
GRADE IV: Laceration through the corticomedullary junction towards the...

Fig. 32:
GRADE V: Kidney shattered or Avulsion of the renal pedicle.