Type:
Educational Exhibit
Keywords:
Metastases, Image verification, Cancer, Imaging sequences, Education, Diagnostic procedure, MR, Oncology, Neuroradiology spine, CNS
Authors:
M. Marinkic, D. Zadravec; Zagreb/HR
DOI:
10.26044/ecr2019/C-3195
Background
Metastases to the spine involving the bones are often diagnosed since they are the third most common site for metastatic disease,
following the lung and the liver.
We discuss here less common sites of spinal metastases which often represent a diagnostic challenge.
With that in mind,
the three possible locations for spinal metastases are intradural intramedullary,
commonly shortened to intramedullary,
intradural extramedullary and extradural (Fig.1).
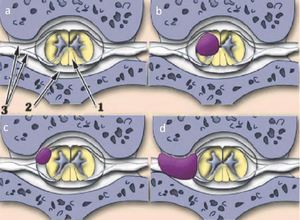
Fig. 1: Location of spinal cord tumors: a) 1 spinal cord 2 dura matter 3 spinal roots b) intradural intramedulllary tumor c) intradural extramedullary tumor d) extradural tumor
Intramedullary spinal metastases are very rare,
occurring in only 0.5-2% cancer patients with advanced disease and comprise 1–3% of all intramedullary spinal cord tumors.
The presence of an intramedullary spinal metastatic lesion suggests an advanced,
biologically aggressive form of cancer.
They commonly occur in the setting of advanced disease and they are almost never the first presentation of malignancy (Fig.2).
The metastatic spread to the spinal cord may result from growth along the Virchow-Robin spaces,
hematogenous dissemination and direct extension from leptomeninges.
In most cases they represent the metastatic spread of lung cancer.
Other primary malignancies that can cause intramedullary metastases are written in the Table.1:
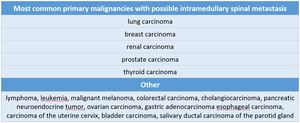
Table 1
It is important to have in mind that there are some primary CNS tumors that may also metastasize to the cord such as glioblastoma,
medulloblastoma and ependymoma.
The most common symptoms in patients with intradural spinal metastases are motor weakness (flaccid or spastic paresis) and dissociated sensory deficits.
Other common presenting features are pain,
bowel or bladder dysfunction and rapid decline in neurological status in elderly patients.
Management of spinal metastasis is undertaken to relieve pain and preserve neurological function.
Therapeutic irradiation,
steroids,
chemotherapy and surgical decompression are available treatment options.
Unfortunately,
the prognosis for this advanced metastatic disease is very poor.

