Metastases to the spine can involve the bone,
epidural space,
leptomeninges,
and spinal cord.
While interpreting spinal cord images it is essential to carefully observe the scans and to detect the exact location of the spinal lesion.
The lesions can be located intradural intramedullary, intradural extramedullary or extradural.
Intramedullary tumors arise within the substance of the spinal cord,
whereas extramedullary tumors are extrinsic to the cord.
The extradural lesions account for up to 95% of spinal lesions and can be divided into pure epidural lesions and those originating from the vertebra extending to the epidural space and subsequently impinging on the thecal sac.
Numerous neoplastic and non-neoplastic processes can be found in these locations and they have to be considered as possible differential diagnoses while analyzing the spinal cord images in patients with suspected lesions (Table.2).
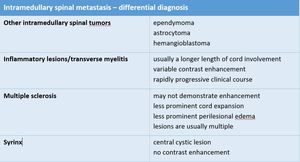
Table 2
Clinical history may provide clues to narrow the differential diagnosis.
For instance,
CSF positive for oligoclonal bands and typical symptoms in a young female adult would favor a demyelinating process.
Osseous metastases in a patient with a known primary malignancy would make an enhancing intramedullary lesion more suspicious for an intramedullary metastasis (Fig.3).
Prominent vascular flow voids along the cord surface in addition to intramedullary edema are helpful in determining if the lesion is a spinal arteriovenous malformation.
MR is considered to be the leading imaging modality in radiographic diagnosis of intradural metastases.
It is most sensitive in assessing changes in spinal cord size and signal intensity changes.
MR of the spine includes the diagnosis of metastasis,
the characterization of the levels of involvement,
and the diagnosis of any associated cord compression.
In some cases CT myelography is preformed since it is a good method for detecting nodular tumor metastases in leptomeningeal metastatic disease.
It is a helpful technique in those patients who cannot undergo an MR (e.g.,
patients with pacemakers,
extreme claustrophobia).
This method is able to detect metastatic disease as thickened nerve roots,
subarachnoid masses,
and/or blockage of the subarachnoid space.
On MR scans all three possible locations of spinal metastases could be assessed (Fig.1).
Some useful tips for detecting each of them are:
- intradural intramedullary metastases expand and cause thinning of the cord around them
- intradural extramedullary masses push the cord away from them,
the dura is seen as a line above them
- extradural lesions occur outside the spinal cord and they displace the thecal sac,
the dura can be seen as a line below the mass
Besides the mentioned locations the metastatic lesions can occur in the osseous spine which is by far the most frequent spinal metastasis location.
Imaging characteristics of intramedullary metastases are illustrated in Table.3,
(Fig.4,
Fig.5 and Fig.6):
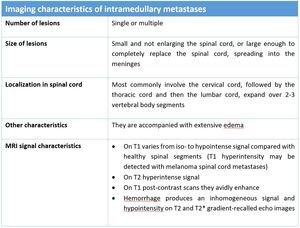
Table 3: Imaging characteristics of intramedullary metastases
T1-weighted sequences are considered the most informative for defining tumor localization and size.
It is practically impossible to determine exact tumor size and borders on T2 weighted images,
because peritumoral edema has a hyperintense MR signal and thus merges with the tumor’s signal.
T1 post-contrast scans are the most important in determining tumor localization and the extent of the infiltrative process in the spinal cord and differentiating the metastatic lesion from other possible spinal lesions (Fig.3 and Fig.6).




