ECR 2019 / C-3212
Splenic lesions in hematologic malignancies: a challenge of imaging diagnosis or not?
Congress:
ECR 2019
Poster Number:
C-3212
Type:
Educational Exhibit
Keywords:
Abdomen, Haematologic, Spleen, CT, MR, Image manipulation / Reconstruction, Contrast agent-intravenous, Puncture, Haematologic diseases, Haemorrhage, Abscess
Authors:
A. VOICOVICI1, A. Dijmarescu2, E. M. Preda2, C. Dumitrescu3, I. G. Lupescu2; 1Bucuresti/RO, 2Bucharest/RO, 3Bucharest, romania/RO
DOI:
10.26044/ecr2019/C-3212
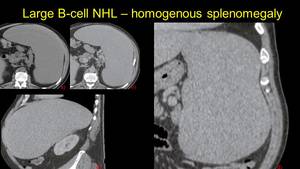
 NECT and b) CECT axial view, images c) and d) sagital and coronal view.")
Fig. 1:
Homogenous Splenomegaly in a pacient with B cell non-Hodkin lymphoma. Image a)...
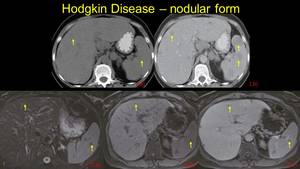
, but with multiple visible miliary nodules after contrast enhancement - axial and coronal view (b and c) - arrows. Note the presence of the peritoneal fluid - asterix")
Fig. 2:
Another pacient with B cell Lymphoma, with homogenous splenomegaly on NECT...
 low intensity signal in T2w with fat saturation images; I.b) intermediate signal in T1 nonenhanced images; I.c) low gadolinium uptake after contrast enhancement. CT examination 3 years after treatment II.a) hypoattenuating, hypoenhancing multiple lesions with modified topography, asociating enlarged lymph nodes in the splenic hillum – disease relapse is considered")
Fig. 3:
Pacient with B cell non-Hodkin lymphoma – MRI diagnosis examination -...
")
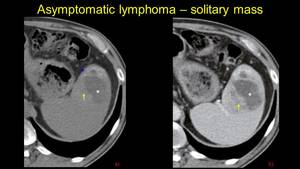
Fig. 5:
A case of Hodkin’s lymphoma, CT examination at diagnosis, and MRI...
 nonenhanced hypoattenuating lesion, b) contrast enhanced CT reveals an enhanceing heterogenous solitary lesion – lymphoma is confirmed by medulary bipopsy.")
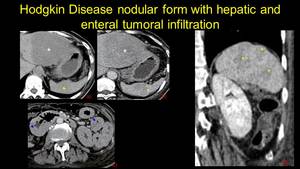
Fig. 4:
Pacient known with cirrhosis. Echography finds an incidental heterogenous...
 hepatic - asterix and b) splenic - arrow hypodense contrast enhanceing lesions; c) duodenal and enteral tumoral implication - arrowhead and d) note that in the coronal view the spleen has normal size.")
Fig. 6:
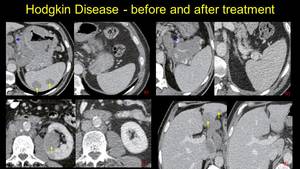
Hodkin lymphoma – a) hepatic - asterix and b) splenic - arrow hypodense...
 – a and b; left kidney tumor (arrow) and retroperitoneal adenopathic block – image c), and finally liver lesions – image d). On the right of these images we note the complete regression at 1 year after the treatment.")
Fig. 7:
Aggressive Hodkin disease, at diagnose presents splenic involvement,...

Fig. 8:
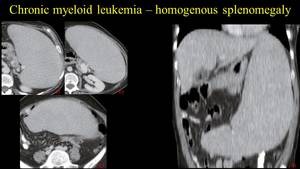
Chronic myeloid leukemia – homogenous splenomegaly – axial view at the...

Fig. 9:
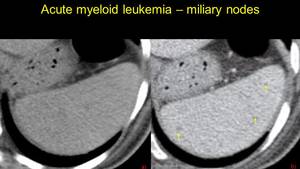
Pacient with acute myeloid leukemia – multiple isodense hypovascular splenic...
 isodense on NECT, b) hypovascular on CECT, which associates a mediastinal tumoral mass.")
Fig. 10:
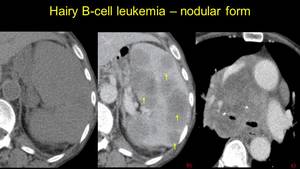
Nodular splenic lesions in a Hary B cell Leukemia – a) isodense on NECT, b)...
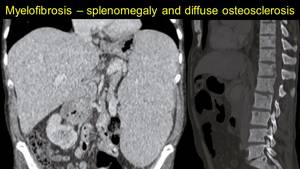
 and diffuse osteosclerosis (image b).")
Fig. 11:
In myelofibrosis, the bone marrow is replaced by fibrotic tissue, causing the...
 that suggest extramedullary haematopoiesis.")
Fig. 12:
Pacient diagnosed with myelodysplastic syndrome performes a CT examination for...
 – images a and b. No signs of acute bleeding after contrast administration (image c). Splenectomy is performed and the hystopathological exam confirms the hematoma with capsular rupture.")
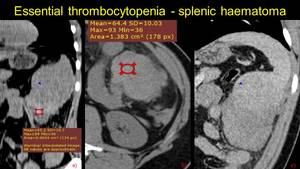
Fig. 13:
We mentioned before the essential thrombocytopenia. We present the case of a...
 axial NECT – fluid accumulation (arrowhead) with b) spontaneous hyperattenuating areas, which in coronal view c) extends on a length of 30 centimeters associating parenchimal compresion (asterix) – degraded subcapsular haematoma, no extracapsular effraction")
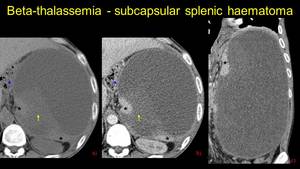
Fig. 14:
Pacient known with beta-thalassemia – a) axial NECT – fluid accumulation...
 with extracapsular effraction (asterix), NECT - a and CECT – b, asscoiating haemoperioneum at pelvic level – c. Note the triangular hipodense lesions – d, unenhancing – e, suggestive for splenic infarction")
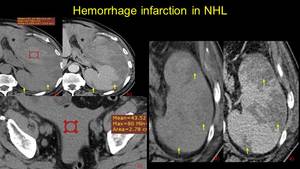
Fig. 15:
Non-Hodkin lymphoma. Splenic spontaneos hyperdense accumulation (ROI) with...
, unenhancing, sugesstive for splenic infarction (arrows), and another hypodense area, slighthly enhancing in venos phase – arrowhead (b) which is homogenized in the parenchymal phase – suggestive for a perfussion disorder.")
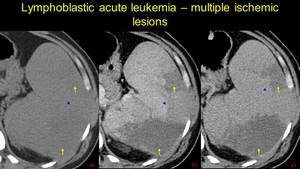
Fig. 16:
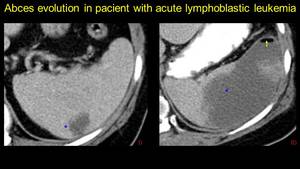
Acute lymphoblastic leukemia known patient. Triangular spontaneos...
, and CECT (b) – asterix. II after 2 years, reevaluation CT shows chronic lesions – arrowhead, with decreased dimensions and capsular retraction with thin fibrotic area – arrow.")
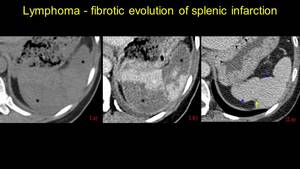
Fig. 17:
Pacient known with lymphoma, presents at the emergency room for upper left...
 and middle of the spleen (NECT – I.c and CECT – I.d). Four years later, disease relapse is suspected – chronic aspect of the infarction with fibrotic bands and capsular retraction. Note the enlarged spleen and peritoneal fluid.")
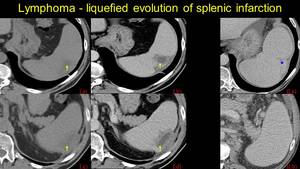
Fig. 18:
Pacient known with Non-Hodkin Lymphoma – liquefied splenic infarction at the...
, with enhanceing thick walls, and fat stranding (arrowhead) – splenic abscess with Candida Albicans.")
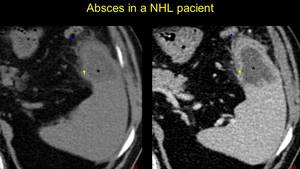
Fig. 19:
NHL pacient presents at the emergency room with fever, chills and pain –...
 – antibiotic treatment for five days is performed, but because of bad evolution, another CT exam for reevaluation is decided – image II – fulminant progression of the absces, with gas-fluid level (arrow). Interventional drainage is practiced – Meticillin resistant Staphylococcus Aures)")
Fig. 20:
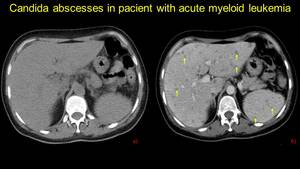
Pacient known with acute lymphoblastic leukemia: image I – splenic abscess...
 and CECT (b) – izodense hypoenhancing lesions suggestive for abscesses and microabscesses – blood tests confirm Candida Albicans")
Fig. 21:
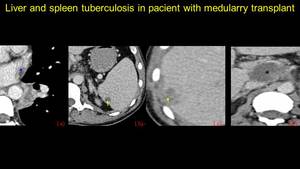
Acute myeloid Leukemia in treatment with cytostatics, presents at the emergency...
, I.b – hypovascular splenic and I.c - liver lesions and I.d – a necrosing adenopathy. A liver biopsy is performed for the lesion in segment VI and the result is liver tuberculosis. The patient is treated in a dedicated hospital and after one year, a reevaluation CT is performed: note the liquefied aspect of the hepatic and splenic lesions and the regression of the hepatic hillum adenopathy.")
Fig. 22:
Pacient who underwent medullary allotransplant, presents at the emergency room...
 lung window, b) mediastinum window – enhancing macronodular tumor with mediastinal adenopathy. Images c and d – NECT and CECT – metastases in the liver and spleen.")
Fig. 23:
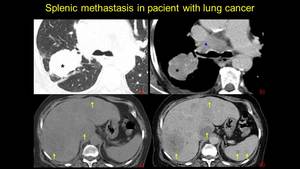
Female pacient known with pulmonary tumor, post-chemotherapy evaluation: - I a)...
 lung window – difuse interstitial pulmonary infiltrates, b) CECT mediastinum window – multiple enlarged limph nodes at the pulmonary hillum (arrowhead), c) multiple hypovascular splenic nodules.")
Fig. 24:
Pacient known with pulmonary and splenic sarcoidosis. A) lung window – difuse...
")
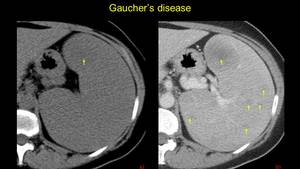
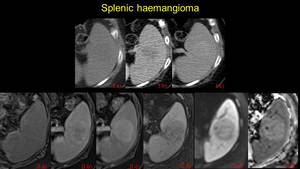
Fig. 25:
Female pacient known with Gaucher’s disease – heterogenous spleno-megaly...
 hypoattenuating spontaneous, with centripete enhancing in venous phase (b), silghtly hyperenhancing in late phase. II MRI examination: a) isointense on T1w images, with similar enhancing pattern (b, c), low signal T2fs (d) and high signal on DWI and ADC (e and f) – splenic haemangioma.")
Fig. 26:
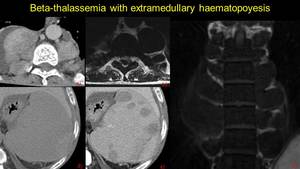
Pacient with hyperecogene lesion identified by ultrasound. I CT examination:...
 CECT axial, b) MRI T2w axial and c) MRI T1w coronal view and splenic extramedullary hematopoiesis – NECT d) and CECT e) in axial view")
Fig. 27:
Pacient know with beta-thalassemia – nodes of paravertebral extramedullary...