Herein we propose a step by step overview that can help poor experience radiologists avoiding misdiagnosis in the evaluation of oncologic CT examination.
Summary is shown in Table 1.
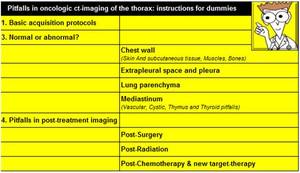
Table 1: Summary
1.
Basic acquisition protocols
Knowledge of main standard CT acquisition protocols,
post-processing techniques and artifacts that can occur is imperative for avoid misdiagnosis and correctly guide staging and treatment of oncologic patients.
Contrast enhancement CT represents the most used technique in oncology field to better recognize tumoral lesions,
to define their anatomical relationships,
to detect metastases and to characterize tumor vascularization and perfusion.
The choose of the correct contrast-enchanced phase depends on the pathology we are looking for but,
typically,
a hepatic or late portal phase (50-60 sec after injection) alone or in association with a late arterial phase (15-20 sec) could be suitable for a satisfactory evaluation.
Non-enhanced CT may be helpful in detecting calcifications,
fat components but it usually performed only for first evaluation.
A minimum of five window settings (soft tissue,
lung,
bone,
liver and vascular) is required to correctly review scans and optimize reporting technique.
Maximum Intensity Projections (MIP) for lung nodules evaluation and Multiplanar Reconstructions (MPR) are also recommended.
2.
Normal or abnormal?
Herein we have segmented thorax in anatomical units describing for each one normal CT appearance and underling potential diagnostic pitfalls.
Chest wall
The evaluation of the chest wall in oncologic field is usually aimed at identifying metastasis or tumor invasion.
Thoracic wall is composed by several structures easily recognizable in CT.
Skin And Subcutaneous Tissue
Often skin is overlooked because of its peripheral location and the so called "attention theft" by the principle lesion.
It is important to look at it,
especially in some kinds of tumor such as melanoma,
and discriminate benign from suspicious lesions.
On CT imaging skin is represented as a thin hyperdense layer with normal thickness less than 3mm.
Hypodense subcutaneous tissue is well detected consisting in collagen and fat tissue
Most skin metastases present as intradermal nodular lesions and only the presence of contrast enhancement helps to differentiate them from benign lesion.
Thickening of the skin is also common in oncology patients and can be a diagnostic challange.
Clinical assessment is useful as it is often due to irradiation or to post-therapy skin reaction.

Fig. 2: Axial contrast-enhanced CT image shows breast skin thickening after radiotherapy in a patient with breast cancer.
Muscles
Intercostal muscles
There are classically described three main intercostal muscles from superficial to deep: the external,
the internal and the innermost intercostal muscles.
They are located in the intercostal space together with the intercostal neurovascular bundles that course under the low margin of the upper rib,
separated by fat tissue.
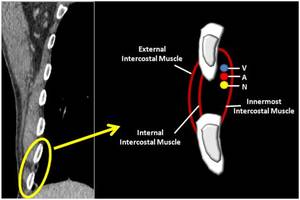
Fig. 3: Coronal CT image (on the left) and a schematic representation (on the right) of intercostal space normal anatomy(V: intercostal Vein, A: intercostal Artery, N: intercostal Nerve).
It is important to remember the presence of these anatomic structures in order to correct diagnosis benign pathologies that could occur and mimic malignancy such as a neurinoma of the intercostal nerve.
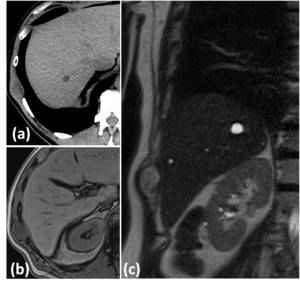
Fig. 4: Imaging features of intercostal nerve neurinoma. (a) Axial non-enhanced CT shows a relative hypodense lesion in the intercostal space between intercostal muscles. MRI is useful for diagnosis: axial T1 out-of-phase (b) and coronal T2 WI (c) reveale typical signal intensity of an intercostal nerve neurinoma.
Diaphragm
Diaphragm represents the most important inspiratory muscle,
has a dome shape and presents several pillars attached to vertebras and thoracic wall.
Sometimes diaphragmatic pillars can mimic solid nodules and multiplanar reconstructions appear necessary.
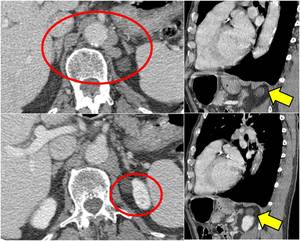
Fig. 5: Axial contrast-enhanced CT at the level of last dorsal vertebra shows the presence of multiple para-vertebral and para-aortic nodularities; on sagittal plane they reveal to be diaphragmatic pillars except for one, more hypodense that reveals to be a kidney cyst.
Dorsal muscles
Dorsal Lipoma
Intramuscular lipomas are very common findings in the chest wall,
they appear as a well defined,
low attenuation mass in the contest of the muscles and may invade and interdigitate the muscle bundle,
resulting in a characteristic striated aspect.
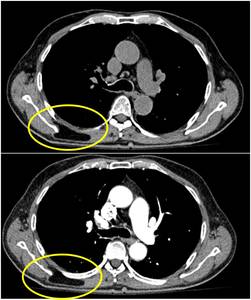
Fig. 6: The figure shows an example of intramuscular lipoma in the contest of the right rhomboid major and trapezius muscles.
Elastofibroma dorsi
Elastofibroma dorsi is a benign asymptomatic soft-tissue tumor,
usually located in the subscapular region.
It is not well defined on CT imaging with density similar to adjacent skeletal muscles and only focal thickening of periscapular tissue can be detectable.
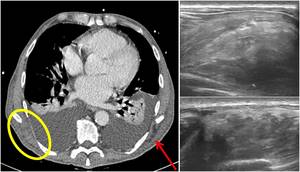
Fig. 7: Axial contrast-enhanced CT image (on the left) shows a focal thickening of right periscapular tissue, better visible if compared with controlateral (red arrow). US evaluation (on the right) demonstrates a well defined multi-layered structure with linear hypoechoic areas intermixed with echogenic areas: typical features of an elastofibroma dorsi.
Bone
Focal bone lesions are frequently encountered in routine imaging studies and often are "left alone" lesions mimicking a tumor or a metastasis.
There are various processes that be confused with bone malignancy but most common lesions are usually represented by normal variants,
congenital or developmental abnormalities,
post-traumatic lesions,
infection and bone involvement in a systemic pathology such as a metabolic process.
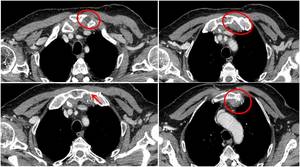
Fig. 8: Follow-up axial contrast-enhanced CT of a patient with a history of prostate cancer shows a nodular hypodense not enhancing lesion at the sternoclavicular joint that causes bone erosion and swelling of joint capsule. It was a sternoclavicular joint arthritis.
Among differential diagnosis for a humeral ill-defined osteolytic lesion,
radiologist should keep in mind the so called humeral pseudocyst,
a normal area of decrease in the trabeculae,
often associated with an increase in fat tissue.
Post traumatic physiological changes such as bone healing can mimic a lesion,
especially in a patient with other metastasis.
Particular attention should be paid to fractures of the ribs that are quite frequent.
Clinical assessment is essential and follow-up images can be resolutive.
Extrapleural Space And Pleura
Extrapleural space is the space localized between the inner surface of the ribs and parietal pleura which is not considered as much as other anatomic entities but in oncologic field few times is involved.
Normally extrapleural space is characterized by adipose and connective tissue,
lymph nodes and vessels.
The evaluation of extrapleural space can be useful as it could present indirect signs of pleural involvement both in malignant or in benign pathologies.

Fig. 9: Axial contrast-enhanced CT image of a patient with a history of lung cancer; bilateral thickening of the extrapleural adipose tissue is showed, more on the left (red arrow) at the level of pleural effusion.
Solitary fibrous tumor of the pleura
Also known as pleural fibroma, it is a rare benign pleural tumors that can be in differential diagnosis with other pleural masses,
in particular on unenhanced CT where it shows low attenuation like other entities,
potentially malignant.
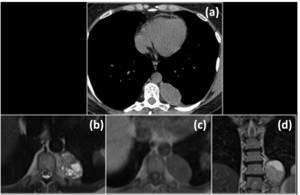
Fig. 10: The figure shows a case of a pleural thymoma metastasis.(a) Un-enhanced CT shows a well defined pleural hypo-isodense mass that seemed a benign lesion. MRI better characterize the lesion: (b) axial T2 WI, (c) axial T1 WI and coronal T2 (d) show intralesion component. It was a metastatic thymoma.
Lung Parenchyma
Familiarity with benign pulmonary conditions that can mimic lung cancer or lung metastases is crucial as misdiagnosis can have major clinical impact.
Rounded atelectasis
Rounded atelectasis is an unusual type of lung atelectasis due to an infolding of redundant visceral pleura that may give a mass-like appearance on CT.
Imaging features that can help in differentiating from malignancy are:
- typical subpleuric location with thickening of adjacent pleura,
- the so called "comet tail sign" due to the stretching of bronchovascular structures,
- typical parenchymal enhancement.
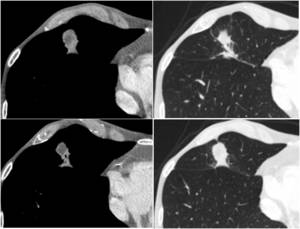
Fig. 11: An example of rounded atelectasis with typical imaging features: subpleuric location with thickening of adjacent pleura and the "comet tail sign" due to the stretching of bronchovascular structures.
Pulmonary hamartomas
Pulmonary hamartomas are very common benign tumors of the lung,
composed of cartilage,
connective tissue,
muscle,
fat,
and bone.
CT imaging shows a well-circumscribed mass with soft tissue attenuation,
containing some areas of fat density and typical popcorn calcification.
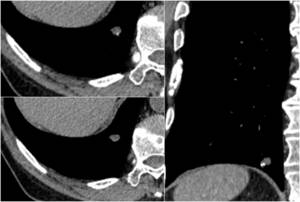
Fig. 12: An example of pulmonary hamartoma.
References: Radiology, Galliera Hospital - Genoa
Infection disease
Infection disease manifesting as a focal opacity such as lung abscess,
atypical pneumonia,
aspergilloma or mycobacterium tuberculosis infection should not be confused with malignancy.
Clinical assessment is essential.
Mediastinum
Vascular Pitfalls
Vascular anatomic variants
Vascular anatomic variants of the thorax represent an incidental findings during CT evaluation of oncologic patients and sometimes may bring misdiagnosis presenting as a mass-like lesion,
especially in axial plane and moreover if tortuosities are present.
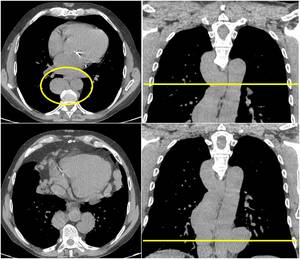
Fig. 13: A case of important dilatation and tortuosity of azygos and emi-azygos veins due to congenital agenesis of inferior vena cava. Axial Unenhanced CT could be challenge showing nodular-shaped paravertebral tissue, mimicking a more common lymphatic pathology.
Table 2 summarize more frequent vascular anatomic variants incidentally found in CT imaging of the thorax.
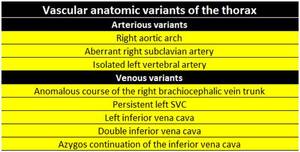
Table 2: More frequent vascular anatomic variants incidentally found in CT imaging of the thorax.
Intrathoracic extramedullary hematopoiesis
Extramedullary hematopoiesis is a rare condition characterized by the presence of extramedullary hemopoietic tissue as a compensatory mechanism in bone marrow dysfunction.
Thoracic localization are quite frequent and can appear as tumor-like masses.
Clinical assessment is essential.
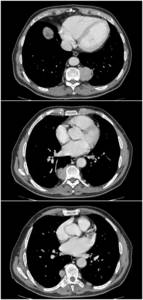
Fig. 14: An example of extramedullary hematopoiesis: axial contrast-enhanced CT shows multiple paravertebral nodular lesion with heterogeneous density in a thalassemia patient.
Cystic Pitfalls
Pericardial recesses
Pericardium is invaginated between the heart and great vessels forming sinus and recesses.
Pericardial recesses can be confused with pathologic mediastinic lymphnodes.
They can be recognized for their anatomical location,
typical fluid attenuation,
focal nature and the lack of mass effect.
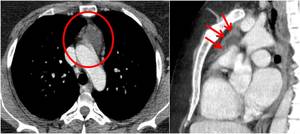
Fig. 15: An example of enlarged pericardial recess that mimics mediastinc lesion. On sagittal plane pericardium can be easily detected all around the fluid attenuated structure.
Pericardial cyst
Pericardial cysts are benign congenital anomalies of the anterior and middle mediastinum.
On CT evaluations they appear as rounded mass with fluid density,
non-enhancing,
just next to the pericardium.
Pericardial cysts can be distinguish from pericardial recesses for localization.
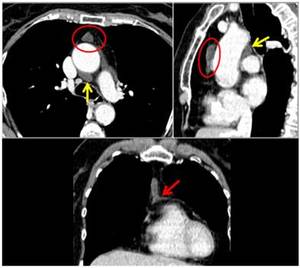
Fig. 16: An example of pericardial cyst in the anterior mediastinum. A thin fat cleavage is recognizable between cyst and aortic pericardium; note the difference with the posterior pericardial recess (yellow arrow). Pericardial connection is seen in coronal reconstructure.
Cisterna Chyli
The cisterna chyli is a dilatation of the lymphatic channels located in the retrocrural space.
It should be recognized and distinguished from retrocrural adenopathy.
Low attenuation,
tubular configuration,
and lack of intravenous contrast enhancement are main imaging feature and sometimes it is challenge because of the possibility of a colliquative lymphnodes.
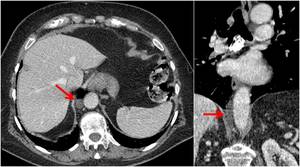
Fig. 17: Imaging features of cisterna chyli.
Esophageal diverticuli
Zenker diverticulum is the most common of esophageal diverticuli and when filled with fluid,
it should not be confused with malignancy.
When in doubt,
typical location should think about it,
multiparametric reconstruction and comparing prior studies could help.
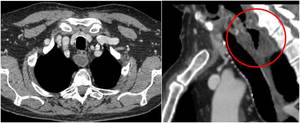
Fig. 18: Axial contrast-enhanced CT image shows a rounded retroesophageus structure with a hyperintense rim and a hypodense core; sagittal plane reveals the presence of a communication with the esophagus and suggests the diagnosis of a Zenker’s diverticulum.
Tracheal diverticuli
Tracheal diverticuli are usually incidental findings,
typically located in the posterolateral tracheal wall at the level of the thoracic inlet.
When filled with air they may mimic pneumo-mediastinum.
A communicating channel with the trachea can bring to the correct diagnosis.
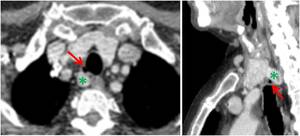
Fig. 19: Axial and sagittal contrast-enhanced CT images show a case of a tracheal diverticulum in a typical location at the right posterolateral tracheal wall (red arrow). A thyroid multinodular goiter extended into the mediastinum is also present, with a digitiform extension that in axial plane can mimic adenopathy (green asterisk).
Cystic tumor degeneration
It is important to remember that some malignant tumor can undergo cystic degeneration like thymomas,
thymic carcinomas,
Hodgkin disease,
germ cell tumors,
mediastinal carcinoma.
It can be very challenge on CT imaging,
especially if a non contrast enhanced CT is performed; further imaging technique should be sometimes required (e.g.
MRI).
Thymus Pitfalls
The eventually of benign thymic enlargement must be known and not be confused with malignancy.
Thymic hyperplasia or the so called rebound hyperplasia,
represents an enlargement of a normally structured thymus,
more common in children,
but frequently found also in adults,
especially after chemotherapy.
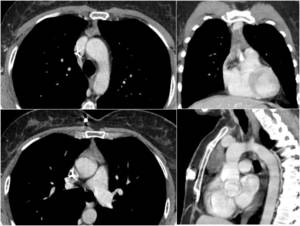
Fig. 20: CT imaging of a thymic hyperplasia (rebound hyperplasia) in a patient after first cycle of chemotherapy (port-a-cath is visible in SVC). At follow-up imaging thymic volume regression was shown.
Thyroid Pitfalls
Thyroid multinodular goiter is a very common disease and often it extend into the mediastinum and should be distinguish from pathologic adenopathy.
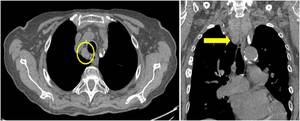
Fig. 21: Non-enhanced CT shows an example of thyroid multinodular goiter extended into the mediastinum that in axial plane should distinguish from adenopathy; coronal plane can help recognizing thyroid morphology.
3.
Pitfalls in post-treatment imaging
Post-Surgery
Surgical techniques that can be used for lung tumor resection include wedge resection,
segmentectomy,
lobectomy or bi-lobectomy and pneumonectomy.
The knowledge of surgical procedures performed is essential to correctly understand post-surgical appearance.
Tracking the course of bronchus and vessels and the presence of surgical material such as surgical clips can be helpful in determining type and location of surgical procedures.
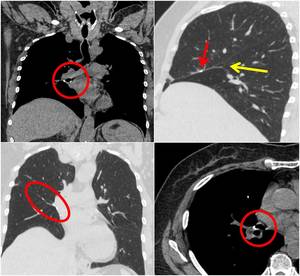
Fig. 22: Example of right middle lobe lobectomy. Surgical procedure can be recognized thanks to the presence of surgical clips at the level of right middle lobe bronchus and along surgical margin in correspondence of right middle lobe localization. Sagittal plane shows the obliteration of the little scissure (yellow arrow).
Wedge resections not include bronchus and artery exportations and typically are recognizable for the presence of a peripheral suture line surrounded by some fibrotic streaks.
In segmentectomy,
lobectomy and pneumonectomy the corresponding bronchus and artery are removed and a muscular graft from intercostal muscle can be used to reinforce surgical wedge.
This graft should not be confused with pleural thickening.
After few time it can calcify.
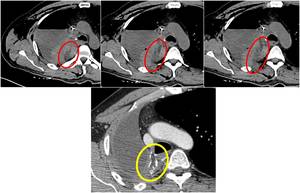
Fig. 23: Example of a right pneumonectomy with muscular graft (from intercostal muscles) used to reinforce surgical wedge. First row of images show the first post-surgical evaluation where muscular graft appears hypodense (red circles). Lower image from a follow-up contrast-enhanced CT shows peripheral calcification of the muscolar graft (yellow circle), just adjacent to surgical cable.
In pneumonectomy heart and mediastinum appeared shifted and sometimes some stretched structure could mimic pathologic adenopathies.
Another particular post-operative finding that can be seen in lung surgery is lung herniation,
the protusion of lung parenchyma beyond the confines of the thoracic cage due to thoracotomies.
.
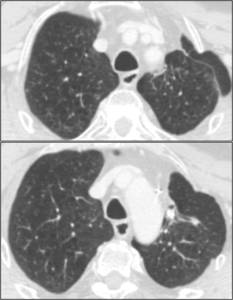
Fig. 24: Example of lung herniation.
Last but not least,
local inflammatory reactions in response to surgical material used it is always to be considered,
not to misdiagnosis tumor recurrence.
Clinical setting and follow-up imaging are useful.
Post-Radiation
Post-radiation changes can be frequently visible on CT imaging and can involve skin and other soft tissues,
lung parenchyma,
the esophagus and bone.
Thickening of the skin is often seen as a normal reaction after radiation treatment.
Fat necrosis within the breast is a pathologic entity that can occur after surgery followed by radiotherapy.
Typical CT appearance is an ill-defined,
speculated mass-like area that change with time with progressive calcification.
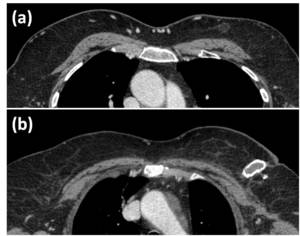
Fig. 26: Two example of breast fat necrosis follwing radiotherapy in patients with a history of left breast cancer. The typical appearance is a ill-defined mass-like area that change with time, hypodense at the beginning (a), with progressive calcification (b).
Typical appearance of lung post-radiation changes includes ground-glass or consolidative bundles opacities and is confined to the radiation treatment plan.
These features help not to confuse normal post-radiation changes with parenchymal pathology.
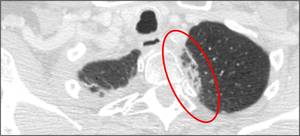
Fig. 27: An example of lung post-radiation with consolidative bundles opacities confined to the radiation treatment plan.
Sometimes fibrosis can occur associated with volume loss,
pleural thickening and shift of mediastinic structures.
Bone alteration can also be detectable after radiation mimicking metastatic disease as it can present as a sclerotic bone lesion.
Sometimes fractures or osteomyelitis can occur.
Post-Chemotherapy & new target-therapy
Post-chemotherapy changes represent various patterns of tissue toxicity and must be identify and report as soon as possible.
Pulmonary toxicity is quite frequent and include hypersensitivity pneumonitis,
non specific interstitial pneumonitis,
cryptogenic organizing pneumonia and diffuse alveolar damage.
CT evaluation can detect the presence of ground-glass nodules,
reticular or interstitial pattern or consolidative opacities,
sometimes mimicking metastatic disease or tumor recurrence.
Clinical information such as the type of chemotherapy and the timing of last administration can be crucial.
A particular attention should be given to the new immuno-therapies that can bring to the so called tumor pseudoprogression: initial tumor growth after therapy administration,
followed by regression.
It has been proved to be a possible pattern of response to immuno-therapies and radiologists should keep it in mind also to correctly address clinician and wait for further follow-up imaging.
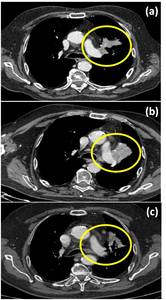
Fig. 29: The figure shows an example of tumor pseudoprogression in a patient with lung adenocarcinoma treated with immuno-therapy. (a) CT scan before starting immuno-therapy; (b) After six months of treatment with Pembrolizumab (anti-PD-1); (c) last control after other six months of immuno-therapy.



 and a schematic representation (on the right) of intercostal space normal anatomy(V: intercostal Vein, A: intercostal Artery, N: intercostal Nerve).")
 Axial non-enhanced CT shows a relative hypodense lesion in the intercostal space between intercostal muscles. MRI is useful for diagnosis: axial T1 out-of-phase (b) and coronal T2 WI (c) reveale typical signal intensity of an intercostal nerve neurinoma.")


 shows a focal thickening of right periscapular tissue, better visible if compared with controlateral (red arrow). US evaluation (on the right) demonstrates a well defined multi-layered structure with linear hypoechoic areas intermixed with echogenic areas: typical features of an elastofibroma dorsi.")

 at the level of pleural effusion.")
 Un-enhanced CT shows a well defined pleural hypo-isodense mass that seemed a benign lesion. MRI better characterize the lesion: (b) axial T2 WI, (c) axial T1 WI and coronal T2 (d) show intralesion component. It was a metastatic thymoma.")






. Pericardial connection is seen in coronal reconstructure.")


. A thyroid multinodular goiter extended into the mediastinum is also present, with a digitiform extension that in axial plane can mimic adenopathy (green asterisk).")
 in a patient after first cycle of chemotherapy (port-a-cath is visible in SVC). At follow-up imaging thymic volume regression was shown.")

.")
 used to reinforce surgical wedge. First row of images show the first post-surgical evaluation where muscular graft appears hypodense (red circles). Lower image from a follow-up contrast-enhanced CT shows peripheral calcification of the muscolar graft (yellow circle), just adjacent to surgical cable.")

, six months after surgery, some subcarenal tissue with a sovrafluid density (40 HU) and low contrast enhancement was noticed. After three months (b) a polypoid lesion appeared in the left principal bronchus. Coronal plane CT (c) shows peri-suture disposition of the suspect tissue. CT-PET was performed a showed midly tissue FDG avidity, but at final diagnosis, made after bronchoscopic biopsy, was a suture granuloma.")
, with progressive calcification (b).")

 in a patient with a history of melanoma. Interruption of therapy and prednisolone administration was resolutive.")
 CT scan before starting immuno-therapy; (b) After six months of treatment with Pembrolizumab (anti-PD-1); (c) last control after other six months of immuno-therapy.")