ECR 2019 / C-3384
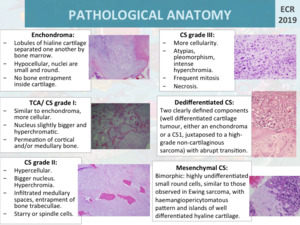
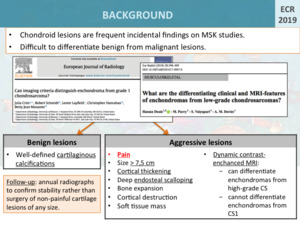
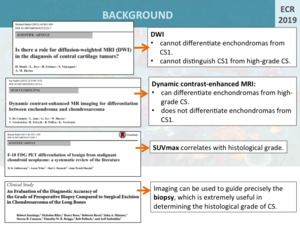
Chondroid matrix lesions: a pictorial review
Congress:
ECR 2019
Poster Number:
C-3384
Type:
Educational Exhibit
Keywords:
Pathology, Neoplasia, Education and training, Education, MR, CT, Conventional radiography, Musculoskeletal joint, Musculoskeletal bone, Bones
Authors:
I. GALÁN GONZALEZ, C. Idoate Ortueta, C. DE BENAVIDES BERNALDO DE QUIRÓS, P. Fernandez Rico, M. J. Moreno, N. Gómez León; Madrid/ES
DOI:
10.26044/ecr2019/C-3384

Fig. 1

Fig. 2

Fig. 3

Fig. 4