Several imgaing Modalities have been used to Diagnose Carotid artery stenosis including:
Carotid duplex (fig 1)
- First line imaging modality for diagnosing carotid artery stenosis because of non-invasive,
available,
low cost with no contrast administration
- The degree of stenosis is determined using B-mode as well as different flow velocities.
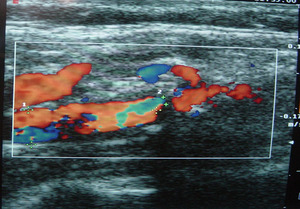
Fig. 1: fig 1. Carotid Doppler showing carotid stenosis with high echogenicity and posterior acoustic shadowing suggestive of calcific plaque causing intraluminal stenosis and flow aliasing.
Table 1 shows how different velocities correlates with different degrees of stenosis.
|
ICA stenosis (%)
|
ICA PSV
Cm/sec
|
ICA EDV
Cm/sec
|
PSV ratio
ICA/CCA
|
|
Normal
|
< 125
|
< 40
|
< 2.0
|
|
<50 %
|
< 125
|
< 40
|
< 2.0
|
|
50-69 %
|
125 - 230
|
40 – 100
|
2.0 - 4.0
|
|
>70 %
|
> 230
|
> 100
|
> 4.0
|
|
Near occlusion
|
variable
|
Variable
|
Variable
|
|
Total occlusion
|
undetectable
|
undetectable
|
Not applicable
|
- Disadvantages is that it is operator dependent and cannot adequately visualize high and low bifurcations.
CTA (fig 2)
- More accurate than carotid doppler because it allows visualization of the high and low bifurcations and not operator dependent,
yet involves radiation exposure,
and contrast injection.
- Even though it is less accurate than Digital subtraction angiography and limited by the presence of circumferential calcifications,
yet it is non-invasive and can visualize the wall of the carotid artery.
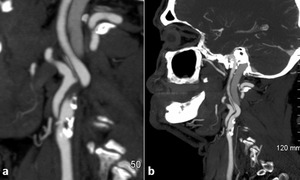
Fig. 2: fig 2. Sagittal CTA showing a calcific plaque causing severe carotid artery stenosis at the ICA origin
MRA and high-resolution vessel wall imaging
- 3D TOF MRA (fig 3) is of comparable accuracy to CTA with no radiation exposure contrast injection,
yet the scan times are relatively longer.
- High resolution vessel wall MRI is a new state of the art imaging modality that can visualize the Plaque components to determine whether they are stable or vulnerable plaques which affect the intervention decision.
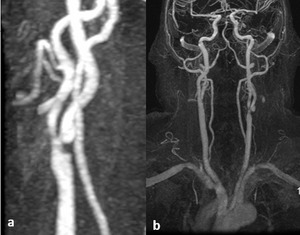
Fig. 3: fig 3. 3D TOF MRA showing severe carotid stenosis in left ICA origin.
Conventional angiography
- Most accurate for luminal assessment,
but because invasive and requires contrast injection with radiation exposure,
it is rarely used for diagnosis and usually reserved for patients undergoing Carotid artery stenting (CAS).
Carotid artery stenting vs end artrectomy
- Carotid artery interventions mainly aim at preventing strokes.
- Until the late 1990s,
it was believed that best medical therapy (BMT) with antiplatelet therapy,
controlling hypertension and hyperglycemia,
stopping smoking and the use of statins to reduce hyperlipidemia cause a significant decrease in stroke risk.
- The first conventional carotid endarterectomy (CEA) was performed by Dr.
Michael DeBakey in 1953 and it was used to treat carotid stenosis,
but it wasn’t until early 2000 that a randomized control trial comparing CEA to BMT North American Symptomatic Carotid Endarterectomy Trial (NASCET),
the European Carotid Surgery Trial (ECST)
- In the North American Symptomatic Carotid Endarterectomy Trial (NASCET),
the European Carotid Surgery Trial (ECST),
it was concluded that Carotid endarterectomy is superior to medical therapy in patients with symptomatic severe carotid artery stenosis >70%.
- As for Asymptomatic patients,
the asymptomatic carotid surgery trial (ACST),
and the asymptomatic carotid atherosclerosis study (ACAS) trials concluded that CEA could be beneficial in patients with stenosis >60%.
- Carotid artery stenting (CAS) as an endovascular alternative treatment approach for CEA was first performed by Marks in 1994.
Several studies were then conducted comparing carotid artery stenting to carotid endarterectomy in treating Carotid artery stenosis.
1.
The SAPPHIRE (The Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy) study
- Enrolled 334 patients with both symptomatic and asymptomatic carotid artery stenosis with 167 patients randomized to CAS and 167 randomized to CEA.
- Primary end point was 30-day stroke/MI death and 1-year ipsilateral stroke or death.
- In first 30 days: 1ry end point was reached in 9.8% vs 4.4%,
but the cumulative stroke,
MI and death were significantly lower in the CAS at 1 year showing 12.2% with CAS vs 20.1% for CEA (p=0.04)
2.
The EVA-3S (Endarterectomy Versus Angioplasty in patients with Symptomatic Severe carotid Stenosis) trial
- Enrolled 527 patients with symptomatic carotid artery stenosis to CAS and CEA with primary outcome being stroke/death which was higher for CAS (11.1%) compared to CEA (6.2)
- The study investigators suggested that “carotid stenting needed to be improved before it could be used as an alternative to CEA in patients with symptomatic carotid stenosis”
3.
The SPACE (Stent-Protected Angioplasty versus Carotid Endarterectomy) trial and ICSS (International Carotid Stenting Study) study failed to prove non-inferiority of CAS compared to CEA due to higher periprocedural complication rates suggesting that CEA should remain the treatment of choice for patients with symptomatic carotid stenosis suitable for surgery.
4.
CREST (Carotid Revascularization Endarterectomy versus Stenting Trial)
- Randomized 2502 symptomatic and asymptomatic patients to CAS and CEA with endpoint being stroke/MI/death during 30-day periprocedural period or ipsilateral stroke within 4 years.
- Showed no significant difference between CAS (7.2%) and CEA (6.8%)
Table 2 shows a comparison between large randomized trial in terms of death/stroke/MI in periprocedural period (defined to be 30 days by most studies)
|
Trial
|
Number of patients
|
Periprocedural D/S
|
P- value
|
Periprocedural D/S/MI
|
P- value
|
|
CEA%
|
CAS%
|
CEA %
|
CAS%
|
|
CAVATAS,
2001
|
504
|
5.9
|
6.4
|
0.8
|
NA
|
NA
|
NA
|
|
SAPPHIRE,
2004
|
334
|
8.4
|
5.5
|
0.36
|
20.2
|
12.2
|
0.004
|
|
SPACE,
2006
|
1200
|
6.3
|
6.8
|
0.09
|
NA
|
NA
|
NA
|
|
EVA-3S,
2008
|
527
|
3.9
|
9.6
|
0.01
|
NA
|
NA
|
NA
|
|
ICSS,
2010
|
1713
|
4.7
|
8.5
|
0.001
|
5.2
|
8.5
|
0.006
|
|
CREST,
2010
|
2502
|
2.3
|
4.4
|
0.005
|
6.8
|
7.2
|
0.51
|
Table 3 shows multiple systematic reviews and metanalysis comparing periprocedural (within 30 days) and long-term results of CAS vs CEA
|
Name
|
Number of studies included
|
Number of patients
|
Periprocedural risk
|
Long term results
|
|
Meier et al.,
2010
|
11
|
4,796
|
Lower risk of D/S for CEA
|
No difference up to 4 years
|
|
Liu et al.,
2012
|
13
|
7,501
|
Significantly higher risk of D/S for CAS
|
No difference up to 1 year
|
|
Bonati et al.,
2011
|
3
|
3,433
|
Higher risk of D/S for CAS
|
Higher 120-day risk of S/D for CAS
|
|
Bonati et al.,
2012
|
16
|
7,572
|
Higher risk of D/S and D/S/MI for CAS
|
Higher 4-year risk of D/S for CAS
|
|
Bangalore et al.,
2011
|
13
|
7,477
|
CAS was associated with a significantly higher risk of D/S/MI and D/S
|
Higher risk of both D/S/MI and D/S for CAS (>40 months)
|
|
Vincent et al.,
2015
|
8
|
7,091
|
Significant higher risk of D/S for CAS
|
Risk of any long-term stroke was significantly higher with CAS (2–10 years)
|
|
Zhang et al.,
2015
|
35
|
27,525
|
Higher D/S risk for CAS
|
Significant higher risk of D/S for CAS at 4- and 10-year but lower risk than CEA at 1-year follow-up
|
D=death,
S=Stroke
- Since the results of stroke/death and MI varied between different studies with most studies suggesting CEA to be superior to CAS in terms of periprocedural death and stroke with CAS superior to CEA in Periprocedural MI,
with variable long term results showing no difference on the long term between both procedures ,
the American college of cardiology (ACA),
American Heart association (AHA),
Society of vascular surgery (SVS),
European Society for Vascular Surgery (ESVS),
European Society of Cardiology (ESC) placed the following guidelines.
Recommend intervention for patients with symptomatic carotid stenosis.
- Support CEA in symptomatic patients with non-occluding carotid stenosis ≥70%
- Do not recommend intervention in symptomatic patients with stenosis <50%.
- They also suggest that anticipated perioperative stroke and death rates should be less than 6% according to the operator’s experience.
- Recommend carotid intervention to be performed within 2 weeks of the onset of neurological symptoms.
As for asymptomatic carotid stenosis,
several ongoing randomized control trials like CREST-2 and ECST-2 are enrolling patients to determine the weather interventional plus medical therapy is superior or inferior to best medical therapy alone with (ACST-2) Asymptomatic Carotid Surgery Trial-2 comparing CAS vs CEA for patients with asymptomatic carotid stenosis.
Different societies suggested that the treatment approach whether using CEA and CAS should depend on plaque characteristics and patient condition and operator experience with CAS suggested for patients with higher risk of CEA and vice versa:
Indication of CAS (high risk patients for CEA based on comorbidities and underlying anatomy)
Comorbidities
- Severe coronary artery disease
- Congestive heart failure
- Recent MI within 6 weeks
- Planned open heart surgery
- Severe pulmonary disease
- Age >80 years.
Underlying anatomy
- Previous CEA or neck surgery
- Very high or very low carotid bifurcations
- Previous radiation
- Bilateral stenosis
- Contralateral carotid occlusion or laryngeal nerve palsy
- Tracheostomy
Contraindications of CAS (depending on plaque morphology and vessel anatomy)
Plaque morphology
- Highly vulnerable plaques (higher risk of fragmentation during wire manipulation): Soft,
lipid rich plaque,
with intraplaque hemorrhage and thin fibrous cap.
- Extensive plaque (>15 mm) plaque
- Heavy calcified plaque
- Preocclusive lesion
- Stenosis at the bifurcation involving both the ICA and ECA
- Lesion located at a curve
Vessel anatomy
- Aortoiliac tortuosity
- Arch type II or III anatomy
- Bovine configuration
- Arch disease
- Proximal or distal ICA tortuosity
Other indications for carotid artery
- Guard against carotid blow out.
- Traumatic pseudoaneurysm or fistula.
- Tandem lesions with intracranial stenosis needing treatment.
- In the settings of mechanical thrombectomy in acute stroke.
- Associated ipsilateral intracranial aneurysms.
All guidelines suggested that procedures should be performed in expert high volume centers with low complication rates
Technique of carotid artery stenting ( Fig. 4 )
- After gaining access via femoral puncture,
the CCA is catheterized and an angiographic image is obtained in the AP and lateral view for the ICA extracranially to determine the degree of stenosis and intracranially to assess for the intracranial circulation.
- A pre-dilatation is performed using a 2-2.5 mm diameter balloon.
(pre-stenting angioplasty).
- A cerebral protection device is navigated across the stenosis and deployed distal to it.
- A stent is deployed across the stenosis (the stent is upsized 1 mm more than the diameter of the carotid with stents used usually between 6 and 9 mm)
- If residual stenosis after stent placement,
post stenting angioplasty is performed using a 5-6 mm balloon.
- A DSA is Performed to insure adequate restoration of flow with no dissection flaps or residual stenosis.
- Cerebral protection device is removed
- DSA in the AP and lateral position is performed for the intracranial and extracranial circulation to ensure no thrombus fragmentation and intracranial embolization.
- During the procedure,
patient is adequately heparinized with 50-70 IU heparin IV bolus per kg.
- Atropine 1 mg is usually administered if post stenting angioplasty will be performed to avoid bradycardia and heart block due to activation of baroreceptors.
- Patient is started on dual antiplatelets (aspirin and clopidogrel) 5 days before the procedure and kept on clopidogrel for 3 months post procedure and aspirin indefinitely.
- The use of embolic protection device is controversial with some studies showing that it might increase the risk of stroke.
If post stenting angioplasty is to be performed however,
it is mandatory to use cerebral protection devices.




 DSA showing severe left ICA stenosis, (b) showing 2.5 mm pre angioplasty balloon navigated across stenosis, (c & d) showing embolic protection device (filter) deployed distal to the stenosis, (e) Ap Native view of Carotid stent after deployment, (f) Post-angioplasty using a 5.5 mm balloon. (g) final control AP DSA showing restoration of the normal ICA caliber.")