Normal anatomy of the penis
The penis is composed of three vascular cylinders.
There are two dorsally located corpora cavernosa and the single ventral midline corpus spongiosum.
Each cylinder is surrounded by a fibrous band,
the tunica albuginea.
The cavernosal bodies communicate with one another through holes in the intercavernosal septum.
The spongiosum may have different signal from the cavernosa because it is functionally a separate space and may have a different rate of vascular flow within its channels than do the cavernosa.
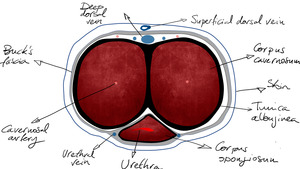
Fig. 2: Axial anatomy of the penis
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
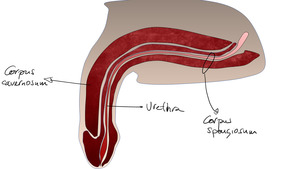
Fig. 3: Sagittal anatomy of the penis
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
The primary source of blood supply to the penis is usually through the internal pudendal artery,
which arises from the anterior division of the internal iliac artery.
The internal pudendal artery becomes the common penile artery after giving off a branch to the perineum.
The branches of the penile artery are the dorsal artery,
the bulbourethral artery,
and the cavernosal artery.
The cavernosal artery gives off many helicine arteries,
which supply the trabecular erectile tissue and the sinusoids.
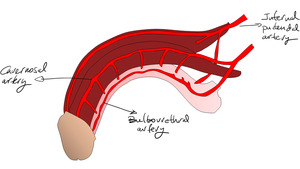
Fig. 4: Arterial anatomy of the penis
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
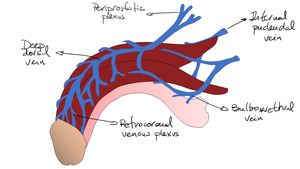
Fig. 5: Venous anatomy of the penis
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
Erection and erectile disfunction (ED)
After an appropriate stimulus,
vascular resistance decreases,
and blood flow through the cavernous arteries increases,
resulting in expansion of blood sinusoids in the cavernosa.
Expansion of the corpora compresses the draining veins in the nonexpendable tunica albuginea,
and penile erection is sustained.
Impairment of theis mechanism renders erectile disfunction,
affecting purely arterial mechanism,
venous or mixed arterial and venous.
Imaging features
The importance of imaging in ED has diminished over the last 2-3 decades because of the poor long-term clinical outcomes of surgery as well as the introduction of oral PDE5-I.
PDE5-I revolutionized ED management,
as a high-quality erection after PDE5-I confirms adequate arterial inflow and effective veno-occlusive mechanisms.
However,
imaging has continued to play a role in the evaluation of non-responders to PDE5-I and in the assessment of cancer patients with ED after pelvic surgery due to prostate or rectal cancer.
Ultrasound is the mainstay imaging modality for evaluating these patients.
It allows to identify and classify the organic component of ED.
Based on the findings on Doppler US,
ED can be categorized into arterial and venous types.
Arteriogenic ED involves impairment of the arterial influx into the cavernosum due to various causes.
In contrast,
an impaired veno-occlusive mechanism causes venous leak,
resulting in what is known as venogenic ED.
Catheter angiography is reserved for those patients with a suspected stenotic or occlusive lesion causing arterial insufficiency.
It is considered a second-line technique utilised as an adjunct to ultrasound.
Catheterisation of the internal pudendal artery allows formal documentation of arterial supply to the penis,
and will demonstrate the extent and location of any arterial lesion as preparation for bypass surgery/revascularisation.
Time-resolved MR angiography (TR-MRA) offers a rapid and noninvasive method for visualizing vascular anatomy and blood flow dynamics.
Several studies have shown that TR-MRA has high sensitivity and specificity,
comparable to conventional angiography,
for detecting anatomic and hemodynamic pathology in a variety of vascular beds.
One technical challenge of TR-MRA is to determine the optimal tradeoff between temporal and spatial resolution to answer the specific clinical question.
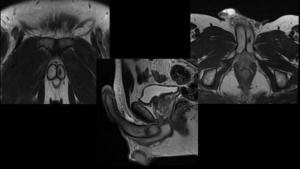
Fig. 6: Patient with ED after a blunt trauma affecting the penis. MRI depicts hypointense and irregular area of 9 mm in T2 weighted image, located in the posterior portion of the left corpus cavernosum, corresponding to fibrous tissue.
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra

Fig. 7: TR-MRA depicts early enhancement of left corpus cavernosum, arising from left internal pudendal artery. The findings are compatible with arteriovenous fistula, secondary to previous trauma.
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
Fig. 8: Same as previous figure, volume MIP rendering depicting the fistula coming from the left internal pudendal artery
References: Servicio Radiodiagnóstico, Clínica Universitaria de Navarra
Advantages of TR-MRA include short acquisition time although with the ability to differentiate between arteries and veins without the pain of estimating contrast bolus arrival times.
Thus,
those cases with confirmed vascular impairment in Doppler ultrasound can be studied trough TR-MRA.
Vascular intervention can be tailored with the data provided with this technique.
TR-MRA technique
All time-resolved MRA methods have at their core a 3D-spoiled GRE sequence with thin slices,
very short TRs and TEs,
low flip angles, use of both read- and phase-conjugate symmetry,
parallel imaging acquisition,
and zero-interpolation filling in the slice direction. Most sequences start using a mask (a full-resolution image) prior to the arrival of the contrast bolus,
so subtracted images can be obtained.
Gadolinium is power injected at a usual rate of 2-3 ml/s.
Accurate timing of bolus arrival is not required (shoot and forget technique!).
The technologist simply starts the sequence and runs it until the contrast has passed through the vascular system.
A smaller dose of contrast can also be used than with conventional CE-MRA due to the higher conspicuity.
Reporting
Reporting information must be precise,
however due to the dynamic information obtained direct consultation through a multidisciplinary approach emerges sometimes as the best option.





