Many extrapelvic pathologies can mimic or cause pelvic masses [1-7].
We have described a variety of these cases including mucocoel of the appendix,
wandering spleen,
Gastric GIST,
Indiana pouch for urinary diversion,
krukenberg's tumour,
hydroureter,
retroperitoneal fibrosis,
etc which at initial presentation were confused as gynaecological origin.
Case 1
• 72 year old female with previous hysterectomy presented with right iliac fossa (RIF) pain.
US demonstrated a large irregular vascular solid mass in the right adnexa (Figure 1) highly suspicious for an ovarian malignancy.
Normal right ovary could not be identified separately on US.
Urgent gynaecology referral and MRI pelvis was performed.
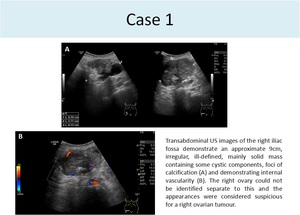
Fig. 1
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• CA-125 (ovarian tumour marker) measurement was normal.
MRI confirmed that the origin of the mass was from a low lying caecum.
(Figure 2).
Right ovary contained a small simple cyst and identified separately adjacent the mass.
(Figure 2).
Histology showed a low grade adenocarcinoma.
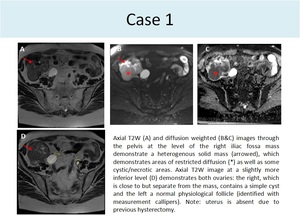
Fig. 2
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
Case 2
• A ‘heterogenous right adnexal mass’ (Figure 3) was identified in a 46 year old female patient who underwent pelvic ultrasound for assessment of early menopause.
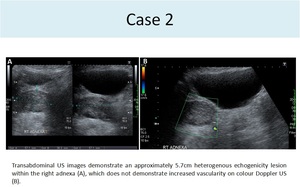
Fig. 3
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• CA-125 was normal.
MRI pelvis was requested to further characterise the lesion.
This demonstrated a tubular mucinous fluid filled structure in the RIF (Figure 4).
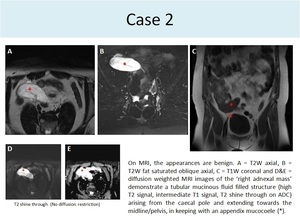
Fig. 4
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• This originated from the caecal pole,
in keeping with an appendix mucocoele.
The uterus and ovaries were normal.
Histology after appendicectomy revealed a low grade mucinous tumour.
Case 3
• 68 year old female referred to gynaecology with abdominal bloating and raised CA-125.
US detected large volume of ascites and a complex,
loculated cystic mass in the right adnexa; possibly a mucinous cystadenoma of the right ovary.
• The patient underwent contrast enhanced CT,
which confirmed gross abdomenopelvic fluid and a fluid-filled tubular structure arising from the caecum suggesting a possible ruptured mucocoele of appendix (Figure 5).
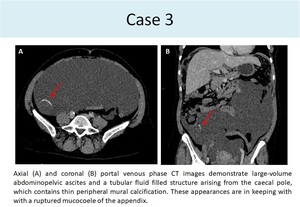
Fig. 5
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
Histology confirmed extensive pseudomyxoma peritoneii in the abdomen originating in the appendix.
• It is important to remember that CA-125 can be raised due to causes other than ovarian malignancy and ascites can be due to a range of aetiologies.
Case 4
• 48 year old female presented with a large ‘suprapubic mass’ which had been gradually increasing in size over a few months.
Initial investigation with US demonstrated a large 12 cm relatively avascular solid-cystic mass with low level internal echoes in close relation to the right ovary (Figure 6),
and was thought to represent a complex right ovarian cyst.
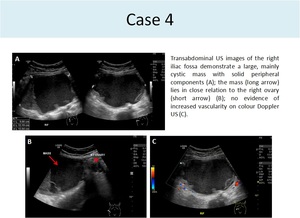
Fig. 6
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• CT showed a large 12 cm cyst with irregular thickened walls in the right iliac fossa likely of ovarian origin.
• Patient had a diagnostic laproscopy.
Uterus and ovaries were normal. A large mobile mass detected attached to the duodenum.
• On careful relook at the CT images with multi-planar reconstruction, the duodenal attachment to mass could be seen retrospectively (Figure 7).
The right ovary containing a follicular cyst was seen to lie separate and inferior to the mass.
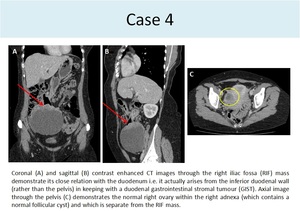
Fig. 7
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• The cyst walls were avid on PET CT (figure 8).
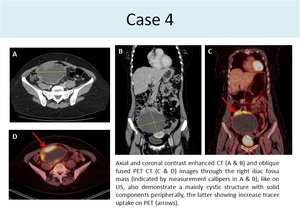
Fig. 8
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• Histology identified a gastrointestinal stromal tumour (GIST; TNM stage T4 N0 M0).
Case 5
• 56 year old female,
with history of Ehler’s Danlos and previous carotid dissection underwent a PET CT for investigation of large vessel vasculitis.
As an incidental finding,
a large high attenuation cystic mass seen,
which appeared to arise from the right adnexa (Figure 9).
Transvaginal US or contrast enhanced CT was suggested to evaluate this further.
• CT was performed first and showed a peripherally enhancing high attenuation cyst within the right adnexa,
which was noted to extend into the mid abdomen (Figure 9),
and gynaecology referral was recommended.
• Subsequent transvaginal US demonstrated a complex cystic right adnexal lesion,
containing septations but no increased vascularity on colour Doppler (Figure 9).
The ovaries were both identified separately to the mass and were normal in appearance.
A differential diagnosis of haemorrhagic right adnexal cyst or hydro/haemato-salpinx was proposed.
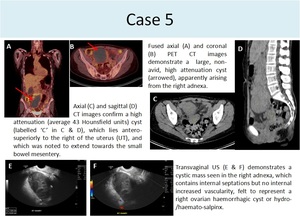
Fig. 9
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• Patient was managed conservatively.
On follow up CT 5 months later,
the cystic structure was markedly reduced in size (Figure 10).
Review of the previous CT images revealed that the lesion was in close relation to the inferior border of the head of the pancreas; and a focus of arterial enhancement was identified within the head of the pancreas,
which was not identified at the time of the initial report. Retrospectively,
putting together the previous appearances,
patient's predisposition for vascular fragility and resorption of the lesion without specific treatment,
a diagnosis of pseudoaneurysm/haematoma from a pancreatic vessel was derived.
This would also explain the appearances on ultrasound.
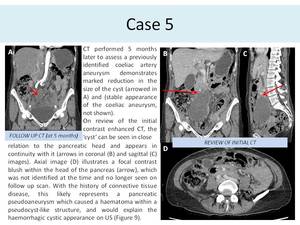
Fig. 10
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• This previous two cases highlight the importance of utilising multiplanar reconstructions particularly when the lesion is large.
These two entities originated in the upper abdomen but on initial imaging masqueraded as gynaecological pathology.
While in one case a careful examination of the previous imaging gave the final answer,
the other was identified on laproscopy.
Case 6
• A 65 year old lady presented with 3 month history of abdominal bloating,
variable bowel habit and reduced appetite.
Contrast enhanced CT showed multiple well defined mixed solid-cystic pelvic masses and only a trace of peritoneal fluid (Figure 11).
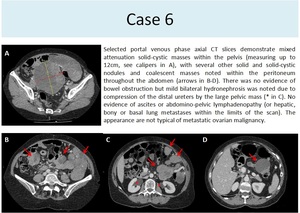
Fig. 11
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
US confirmed the predominantly solid nature of the nodules (Figure 12).
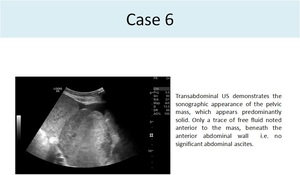
Fig. 12
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• Although reported initially as likely ovarian tumour with peritoneal metastases,
on review at gynaecology MDT,
it was felt that the very well defined predominantly solid appearance of the pelvic mass and peritoneal nodules and very little ascites despite the large peritoneal deposits were not typical features of metastatic ovarian malignancy.
• Biopsy revealed a poorly differentiated malignancy or sarcoma of unknown origin,
in keeping with the imaging findings.
• It is important to consider all imaging features and whether these fit with the clinically suspected diagnosis.
Histological diagnosis is important to guide appropriate treatment.
Case 7
• A large pelvic cyst was initially identified on pelvic ultrasound performed during early pregnancy in a young patient.
It contained low-level internal echoes and few septations but no solid elements or increased vascularity (Figure 13,
A & B),
presumed to be a haemorrhagic cyst related to pregnancy.
It remained stable throughout pregnancy.
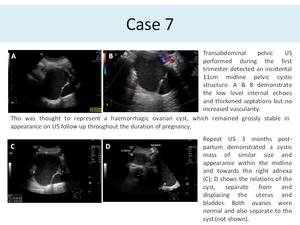
Fig. 13
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• Patient delivered by a Caesarean section and ovaries appeared normal at surgery and was therefore assumed that the cyst had resolved.
• Approximately 3 months post-partum,
the patient developed lower abdominal pain and recurrence of the cyst was suspected clinically. US pelvis demonstrated a septated cystic mass,
containing low level echoes,
in the pouch of Douglas and right adnexa,
similar to the originally described and monitored cyst (Figure 13,
C & D).
The uterus and ovaries were normal.
Given the unclear aetiology,
a CT was performed.
This identified a 14cm cyst in the right adnexa with mildly thickened and smooth hyperenhancing margins.
The right ovary was not positively identified on CT.
• Following discusson at gynaecology MDT ,
an MRI was suggested to more accurately characterise the cyst and assess its relation to the pelvic organs.
MRI confirmed a large pelvic cyst occupying the presacral space (similar to the location marked on initial US (Figure 14) in close relation to the rectum.
Both ovaries were normal and seen separate to the cyst.
The most recent working diagnosis is of a developmental cyst (tail-gut duplication cyst or neuroenteric cyst).
This most likely was present since birth and incidentally identified on the antenatal scan.
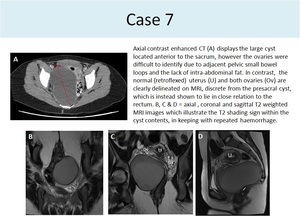
Fig. 14
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
Case 8
• 63 year old female with known Crohn’s disease presented with acute abdominal pain,
vomiting and diarrhoea.
CT showed a fluid and gas containing ‘collection’ within the left hemipelvis,
closely related to a couple of large diverticula arising from the sigmoid colon (Figure 15),
reported as a likely diverticular abscess.
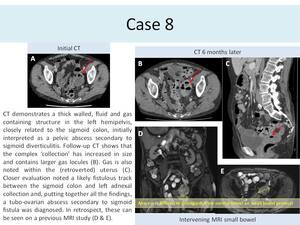
Fig. 15
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• US guided drainage was requested however no drainable collection was identified on US and antibiotic treatment with interval CT was recommended.
• CT 6 months later showed a persistent ‘collection’,
which had increased slightly in size and contained larger locules of gas.
Further inspection identified gas within the uterus and a fistulous connection between the sigmoid colon and left adnexal collection. The images were reviewed by a radiologist with subspecialist interest in gynaecological imaging who recognised the overall features were in keeping with a tubo-ovarian abscess secondary to sigmoid fistula.
• An MRI small bowel study which had been performed during the intervening period (for evaluation of distribution of known Crohn’s disease,
which had been diagnosed abroad) was also reviewed and,
in retrospect,
the left tubo-ovarian abscess can be seen – although,
at the time,
this will have been difficult to appreciate as it would be difficult to distinguish from normal bowel,
especially when the protocol and clinical question were dedicated to evaluate the small bowel.
Case 9
• 50 year old lady presented with pelvic pain refered to gynae clinic after an external ultrasound assessment showed bilateral pelvic masses.
• Staging CT confirmed presence of bilateral ovarian masses with no other obvous abnormality.
(figure 16). Biopsy revealed mucin-producing signet-ring cells,
proving these to be Krukenberg tumours i.e.
ovarian metastases from a gastric primary.
The primary tumour was not identifiable on CT.
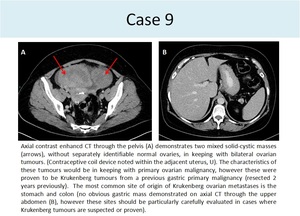
Fig. 16
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
Case 10
• A 48 year old female with previous total thyroidectomy for Graves disease presented with clinical and biochemical evidence of hyperthyroidism. The patient underwent a thyroid 99mTc pertechnetate SPECT-CT scan to look for residual Thyroid.
There was no evidence of residual thyroid in the neck or chest (Figure 17,
A).
Thyroid US showed no sonographic evidence of residual or ectopic thyroid tissue.
• Given her persistent hyperthyroidism,
struma ovarii was considered and US pelvis suggested,
which identified a large complex cystic and solid pelvic mass (Figure 17,
B)
• I 123 Planar and SPECT- CT showed uptake in the cyst walls in keeping with functioning thyroid tissue (Figure 17,
C & D).
• Histology showed follicular carcinoma in a struma ovarii tumour which accounted for the ectopic thyroid hormone production.
• It is important to remember this unusual diagnosis as a possible differential for a malignant-looking ovarian mass,
especially in a patient who may be undergoing investigation for clinical symptoms or signs of hyperthyroidism.
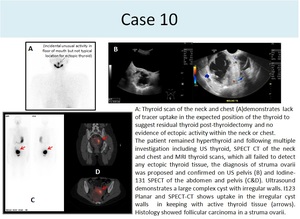
Fig. 17
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
Case 11
• When this young patient with known long standing left adnexal cyst thought to be a hydrosalphynx presented with left iliac fossa pain,
she underwent an MRI and then CT which showed no change in the adnexal cyst but a low abdomino-pelvic homogeneous solid mass.
The mass looked similar in density to spleen (Figure 18).
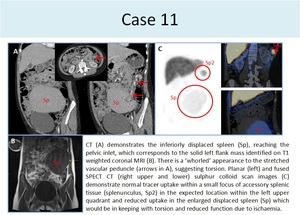
Fig. 18
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• Sulphur colloid scan was performed.
The mass showed uptake in keeping with splenic tissue confirming a diagnosis of a wandering spleen.
The level of tracer uptake in this ectopic spleen was slightly reduced and this was thought to be due to intermittent torsion of the long pedicle which also explained the patient’s presentation with pain (Figure 19).
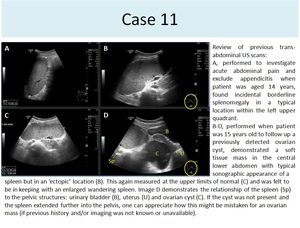
Fig. 19
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• This illustrates the fact that multiple modalities may be required to elicit different information which when gathered together help in arriving at a definitive conclusion.
Case 12
• A 57 year old female underwent pelvic US for investigation of increasing dyspareunia and ‘pelvic pressure’ sensation.
US demonstrated an avascular,
thin-walled tubular fluid-filled structure in the right adnexa,
which was interpreted as a possible hydrosalpynx (Figure 20).
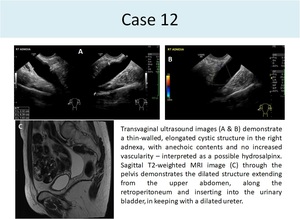
Fig. 20
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• MRI pelvis identified that this was indeed a very distended ureter (Figure 20).
However when Mag-3 renogram was performed,
the right ureter showed no obstruction( Figure 21).
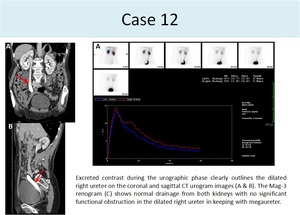
Fig. 21
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• Taken together,
the multiple imaging modalities enabled diagnosis of a right sided megaureter to be made (rather than hydroureter/ hydrosalpynx).
Case 13
• An Indiana Pouch is a form of urinary diversion following cystectomy due to malignancy or trauma [ref ].
It is a surgically constructed neobladder,
formed from the caecum and ascending colon,
connected to the skin via a short segment of ileum.
Figure 22 illustrates the appearance of an Indiana Pouch on whole body bone scan,
with accumulation of tracer.
On MRI,
the pouch has the appearance of a fluid-filled tubular structure,
similar to a segment of large bowel.
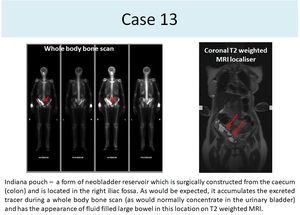
Fig. 22
References: Department of Radiology, Countess of Chester Hospital, Chester, UK 2019
• It is important to be aware of this,
and other,
form(s) of urinary diversion and to always correlate findings with a patient’s history or previous imaging to avoid the potential for misinterpreting these for gynaecological pathology like ovarian cysts or hydrosalpinx.
• A peritoneal inclusion cyst is another cystic structure which could occur in the pelvis and potentially be confused for an ovarian cyst.
Knowledge of patient’s surgical history here is important in this case.






















