Lymph node assessment has always been a challenge for radiologist for proper assessment and staging of malignant diseases and this include different ways using different imaging modalities.
General Lymph nodes assessment
Morphological criteria that can be useful for nodal assessment include [1]:
1.
Nodal size:
Lymph nodes size assessed in the axial short-axis.
This assessment method has limited accuracy and can't differentiate enlarged hyperplastic benign from malignant lymph nodes.
So lymph node size alone is not a reliable parameter [1].
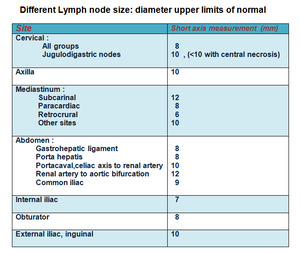
Fig. 12: Table (1) showing upper limit diameters of normal lymph nodes in different body locations
References: Padhani, A R. 2014. “Lymph Nodes.” In Recommendations for Cross-Sectional Imaging in Cancer Management, edited by T Nicholson, Second edi. London: The Royal College of Radiologists.
2.Nodal shape (round or elliptical)
Normally the lymph node is oblong kidney shaped with a fatty hilum and has a smooth outline except for small vessels at the hilum.
Loss of this normal morphology may occur in the presence of metastatic disease [2].
3.Nodal contour (to identify extracapsular spread)
4.Nodal clustering.
5.Nodal density /intensity (particularly cystic or necrotic regions)
Malignant nodes may have heterogeneity on T2-weighted MR images,
as compared with benign nodes.
The presence of a normal fatty hilum more likely indicares a benign node .
Central necrosis in a node is commonly seen with certain types of metastatic disease,
however it is not a specific sign that can be seen also in infection [2].
6.Enhancement characteristics following intravenous contrast medium administration (homogeneous/heterogeneous /central necrosis).
Different imaging modalities used in LN assessment
Ultrasound (US) Fig. 1 Fig. 2
It is a proper assessment tool in cervical ,axillary,
upper abdominal and inguinal Lymphadenopathy.
The doppler can also allow assessment of vascularity.
Endoscopic US (EUS) has also been used to assess regional lymphadenopathy in esophageal,
pancreatic,
and rectal carcinomas.
And it is considered most accurate technique for the locoregional (T and N) staging of esophageal cancer [3].
Normal nodes appear as hypoechoic flat structures with fatty hilum.They may show hilar vascularity but are usually hypovascular.
Malignant infiltration changes the normal US appearance of the lymph nodes,
usually into enlarged rounded nodes with increased vascularity [3].
Cross-sectional Imaging (CT ,MRI) Fig. 3 - Fig. 4
The assessment of lymph nodes using these modalities depends mainly on lymph node anatomy.
On cross-sectional imaging,
a normal lymph node shows ovoid shape with a central fatty hilum having smooth and well-defined border and homogeneous density [3].
Malignant lymph node will be more rounded shape( long-to-short axis ratio decreases) and may show eccentric cortical hypertrophy.
heterogeneous nodal signal intensity or an irregular border [3].
Metastatic nodes may show central necrosis as a hyperintense signal on T2-weighted images (T2WI).
Multiple enlarged lymph nodes associated with conglomeration are highly indicative of nodal metastasis.The higher cell densities in metastatic nodes result in lower ADC values relative to benign lymph nodes which can be furtherly used as a promising tool to detect clinically occult metastatic lymph nodes [4].
PET/ PET-CT Fig. 5 Fig. 13
PET,
or primarily PET/CT in recent years,
has been widely used for initial staging and follow up as it has a high sensitivity in detecting metastatic lymph nodes [3].
The advantage of PET over conventional imaging techniques is its ability to distinguish between viable tumor and necrosis or fibrosis in residual mass often present after treatment even if it has a stable size.Malignant tissues usually present with significantly increased SUV,
which is the single most valuable strength of PET,
due to their higher metabolic rate [5].
Lymph Nodal staging through TNM classification
The TNM Staging System the most commonly used staging system all over the world ,
in order to stage different types of cancer [6].
The TNM Staging System is based on ;
1.The size / continuous extent of the primary tumor (T)
2.The extent of spread to the lymph nodes (N),defined for each cancer site and should include : The absence or presence of cancer in regional node(s),
their number ,
bilateralilty ,
size and extension through the regional node capsule [7].
NX Regional lymph nodes cannot be evaluated
N0 No regional lymph node involvement (no cancer found in the lymph nodes)
N1-N3 Involvement of regional lymph nodes (number and/or extent of spread)
3.The presence of metastasis (M), defined for the presence of distant metastases in sites and/or organs outside the local tumor area and regional nodes as defined for each cancer site [7].
Regional nodal metastases are described by the N stage,
whereas non-regional lymph node metastases are described by M stage (usually M1).
This has a direct impact on overall tumor stage [7].
Lymph node assessment per revised RECIST (rRECIST) criteria
RECIST 1.0 standing for Response Evaluation Criteria in Solid Tumors,
is a guideline formulated to give a standard approach in assessing the solid tumours and their follow up.It considers a maximum of 10 lesions in general and 5 tumor lesions per organ as target lesions which are follow up to get the response of the Tumor to treatment.
In 2009,
a revision for the included criteria was done giving the what is called RECIST 1.1 where the lymph nodes with certain criteria could be included as target lesions and the target lesions were reduced to be 5 in general and 2 per organ in maximum [8,9].
Concerning lymph nodes,
in order to be considered a malignant pathologically enlarged and measurable lymph node must be > or equal to 15 mm in short axis when assessed by CT scan at baseline and in follow-up.They are considered non measurable or non-target when pathological lymph nodes have a > or equal to 10 mm to <15 mm in the short axis.when the short axis is <10 mm,
they are considered non-pathological and should not be recorded or followed [10].(see Fig.6)
Lymph nodes assessment affect the total response of the patient ,
for example Complete response (CR ) by RECIST 1.1 requires,
first,
the disappearance of all target lesions; and,
second,
a reduction in the short-axis measurement of all pathologic lymph nodes (whether target or non-target) to < 10 mm [10].
However ,
a drawback is that RECIST is not applied in malignant lymphoma patients,
for whom alternative international guidelines exists.The new criteria (IWG 2007) were applied to NHL and also Hodgkin's disease [11].

Fig. 6: Target LN according to RECIST 1.1
Assessment of lymphomatous lymph nodes infiltration Fig. 9 Fig. 10
Lymphoma may affect lymph nodes or other body organs.
On US,
lymphomatous lymph nodes appear enlarged ,
rounded,
with homogeneous echotexture yet may appear hypoechoic because of the lymphomatous tissue giving a pseudocystic appearance.
On CT ,They are also seen enlarged with homogeneous density.
Some types of lymphoma subtypes as small cell lymphocytic lymphoma and chronic lymphocytic leukemia may present with a large number of small lymph nodes[13].
Lymphoma Staging is based on the extent of involvement of nodal groups,
as follows:
Stage I: Single lymph node group;
Stage II: Multiple lymph node groups on one side of the diaphragm
Stage III: Multiple lymph node groups both above and below the diaphragm
Stage IV: Non-contiguous extranodal involvement (eg,
liver,
lung,
or bone marrow) [13].
The modified International Working Group response criteria are applied to non-Hodgkin lymphoma and also Hodgkin’s disease.This includes initial and follow up assessment by:
• Clinical assessment
• Bone marrow biopsy
• Whole body CT-scan :The target lesion in CT is measured along two perpendicular planes and to get the product of the diameters (longest diameter × short-axis diameter).
• PET mainly for hypermetabolic lymphomas [12].
A highlight of nodal staging of common regional tumors:
Gentourinary [2,14]:
Perivisceral - Internal iliac - External iliac
Perivisceral - Paraaortic
Inguinal and External iliac * Regional only in setting of previous
scrotal or inguinal surgery.
Perivisceral- Internal iliac - External iliac- Common iliac- Paraaortic
Perivisceral - Internal iliac - External iliac - Common iliac
Perivisceral - Internal iliac - External iliac - Common iliac - Paraaortic
Perivisceral- Internal iliac - External iliac
Renal hilar - Paracaval - Para-aortic - Periaortic (lateral aortic) -
Retroperitoneal NOS
Gastrointestinal [14]
Pericolic/perirectal - Ileocolic - Right colic - Middle colic - Left colic -
Inferior mesenteric artery (IMA) - Superior rectal (haemorrhoidal)
Hepatocellular carcinoma
Hepatoduodenal ligament - Caval lymph nodes - Hepatic artery
Pancreatic cancer
Peripancreatic- Hepatic artery- Coeliac axis - Pyloric
Head and neck cancers spread to neck lymph nodes [15]:
Level I,II,III
Level II,
III,
IV
Level V
Level VI
Level VII
Retropharyneal lymph node

Malignant lymph node - morphology and Doppler analysis.https://radiopaedia.org/cases/malignant-lymph-node-morphology-and-doppler-analysis-1?lang=gb.Retreived on 08.01.2019")
Malignant lymph node - morphology and Doppler analysis.https://radiopaedia.org/cases/malignant-lymph-node-morphology-and-doppler-analysis-1?lang=gb.Retreived on 08.01.2019")
 References: Deb S (2015) Supraglottic squamous cell carcinoma.https://radiopaedia.org/cases/supraglottic-squamous-cell-carcinoma-1.Retrieved on 08.01.2019")
. References: Deb S (2015) Supraglottic squamous cell carcinoma.https://radiopaedia.org/cases/supraglottic-squamous-cell-carcinoma-1.Retrieved on 08.01.2019")
.Relapsed non-Hodgkin lymphoma.https://radiopaedia.org/cases/relapsed-non-hodgkin-lymphoma-2?lang=gb.Retrieved on 08.01.2019")

 and periportal ( yellow interrupted circle)")
")
 Hodgkin lymphoma.https://radiopaedia.org/cases/hodgkin-lymphoma-7. Retrieved on 07.01.2019")
 Hodgkin lymphoma.https://radiopaedia.org/cases/hodgkin-lymphoma-7. Retrieved on 07.01.2019")
associated with multiple metastatic enlarged mediastinal lymph nodes at the upper mediastinum and prevascular group nodes (left orange star) associated with invasion of the superior vena cava and the formation of a tumoral thrombus). References: El-Fiky MM. (2017) Superior vena cava invasion and obstruction.https://radiopaedia.org/cases/superior-vena-cava-invasion-and-obstruction?lang=gb. Retrieved on 08.01.2019")
 showing upper limit diameters of normal lymph nodes in different body locations References: Padhani, A R. 2014. “Lymph Nodes.” In Recommendations for Cross-Sectional Imaging in Cancer Management, edited by T Nicholson, Second edi. London: The Royal College of Radiologists.")
. Papillary thyroid carcinoma. Radiopaedia.org/cases/papillary-thyroid-carcinoma-18.Accessed 11-1-2019")