We present the following clinical cases that turned out to be infrequent -and unexpected- orbital tumors.
Case Nº 1:
24-year-old man with right proptosis.
Figure 1: The initial computed tomography (CT) scan shows a solid right intraconal mass,
isodense to the muscles (A).
It reaches the orbital apex without spreading to the sphenoidal cleft (B,C),
and also contacts and displaces the optic nerve (D).
After contrast administration,
it shows intense heterogeneous enhancement (B,C,D).
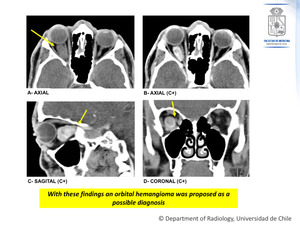
Fig. 1: Case Nº 1:
24-year-old man with right proptosis.
Initial computed tomography (CT) scan.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Figure 2: Contrast-enhanced CT scan,
a year after the initial study.
There is a significant increase in size,
which determines a greater displacement of the optic nerve (B) and greater proptosis (A,C).
The mass now has an extraconal component (B).
No bone erosions are observed.
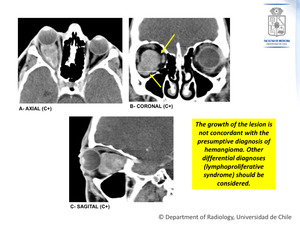
Fig. 2: Case Nº 1:
24-year-old man with right proptosis.
Contrast enhanced CT scan, a year after the initial study.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Figure 3: Contrast-enhanced MRI.
3 years from the initial CT scan.
There has been even more increase in the size of the mass (A,B),
which determines an even greater displacement of the optic nerve (C,D),
even more proptosis and also bone remodeling is now evident.
The mass is markedly hyperintense on T2 (A),
isointense on T1 (B) and there is intense heterogeneous enhancement with gadolinium (C,D).
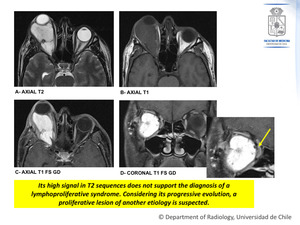
Fig. 3: Case Nº 1:
24-year-old man with right proptosis.
Contrast enhanced MRI. 3 years from the initial CT scan.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Biopsy result: SOLITARY FIBROUS TUMOR,
MYXOID
Generalities:
- Very uncommon spindle-shaped cell tumor of mesenchymal origin that usually arises in the pleura and peritoneum.
- It has recently been identified in various subsites of the head and neck,
including the orbit.
- The use of immunohistochemical markers,
specifically CD34 (hematopoietic progenitor cell antigen),
helps to differentiate this lesion from other spindle-shaped cell tumors of the orbit,
such as fibrous histiocytoma,
hemangiopericytoma,
meningioma,
and schwannoma; it has turned out to be positive in 79% to 100% of cases of solitary fibrous tumors.
Clinical presentation:
- Slow growing,
with an insidious and nonaggressive clinical course.
- Average age at presentation: 40 years.
- No sex predilection.
- Symptoms: Gradual unilateral painless proptosis,
decreased visual acuity,
restricted motility,
palpable orbital mass.
Imaging findings:
- Unilateral,
well-defined mass.
- Most frequently located in the extraconal space (67% approximately),
but can be found anywhere in the orbit.
- It can extend to other spaces outside the orbit (nasal cavity,
base of the skull,
cranial vault).
On CT:
- Isodense to muscles.
- Marked contrast enhancement.
- Bone remodeling can be seen,
without bone destruction.
On MRI:
- T1WI: Homogeneously isointense to gray matter.
- T2WI: Heterogeneously isointense or hypointense (due to fibrous tissue with high collagen content).
- A few cases have shown heterogeneous hyper-intensity or even a cystic appearance,
which may be correlated with the presence of hemorrhage,
myxoid component,
cystic degeneration or fresh fibrous tissue (As in this case,
in which the tumor is a myxoid subtype).
- Presence of tubular flow-voids,
that represent fast-flow vessels.
- Marked enhancement after contrast administration,
due to high vascularity.
In dynamic contrast enhancement studies,
the majority shows a “washout” pattern,
which is helpful in differentiating these lesions from hemangiomas (“progressive” enhancement pattern) and schwannomas (“persistent” enhancement pattern).
Case Nº 2:
55-year-old man,
that presents with left unilateral exophthalmos of one year of evolution and intermittent pain.
Figure 4: Contrast-enhanced MRI.
There is a left intraconal nodular lesion,
that contacts the lower rectus muscle (D).
It is hypointense on T1WI (A) and relatively hypointense on T2WI (B).
After contrast administration,
it shows intense homogeneous enhancement (C,D).
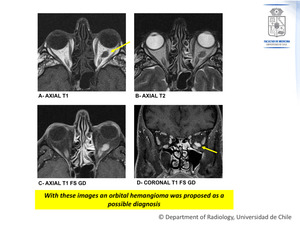
Fig. 4: Case Nº 2:
55-year-old man, that presents with left unilateral exophthalmos of one year of evolution and intermittent pain.
Contrast enhanced MRI.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Biopsy result: NODULAR FASCIITIS
Generalities:
- Benign fibroblastic proliferation.
- Unknown pathogenesis.
There could be a relationship with a trauma history.
- It can develop in any part of the body.
About 15-20% develop in the head and neck.
- Corresponds to <1% of all orbital lesions.
- Wide age range.
- Facial or periorbital involvement is more frequent in the pediatric population than in adults.
- Anterior orbital involvement is more frequent than posterior involvement.
Clinical presentation:
- Unilateral proptosis.
- Fast growth rate.
- Pain.
Imaging findings
- Usually solid and well defined soft tissue mass.
- A cystic component is less frequent.
- Unlike other locations,
it can present itself as an aggressive mass in the orbit.
- Moderate to intense contrast enhancement.
- In MR there is variable signal intensity depending on the histological subtype (myxoid,
cellular or fibrous).
Case Nº 3:
42-year-old woman with mild left proptosis.
Figure 5: The initial CT scan shows a left solid extraconal expansive lesion that contacts the lateral and inferior rectus muscles (A,B).
In the axial plane extension through the inferior orbital fissure to the pterygopalatine fossa and the masticatory space is observed (C).
This lesion shows tenuous enhancement after contrast medium administration (B,C).
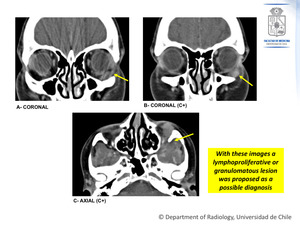
Fig. 5: Case Nº 3:
42-year-old woman with mild left proptosis.
Initial CT scan
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Figure 6: Contrast-enhanced MRI.
4 years from the initial CT scan.
The left extraconal expansive process is seen.
It is isointense on T1WI (A) and heterogeneously hypointense on T2WI (C) and there is moderate enhancement after gadolinium administration (B,D).
There is better demonstration of the extension through the inferior orbital fissure to the infratemporal fossa (D).
Also,
mass effect is noted now,
with a displacement of the infraorbital nerve towards caudal and bone remodeling of the infraorbital osseous component (B).
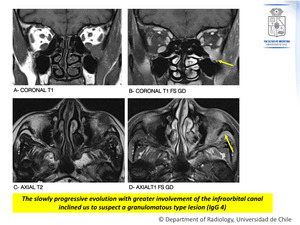
Fig. 6: Case Nº 3:
42-year-old woman with mild left proptosis.
Contrast enhanced MRI. 4 years from the initial CT scan.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Biopsy result: ROSAI-DORFMAN DISEASE
Generalities:
- Also known as “sinus histiocytosis with massive lymphadenopathy”.
- Rare benign entity.
It is a subtype of histiocytosis of Non-Langerhans cells that usually manifests with bilateral cervical adenopathy.
- It mainly affects children,
adolescents,
and young adults.
Clinical presentation:
- Typically,
there is nodal involvement,
so usually,
patients present with bilateral painless cervical lymphadenopathy,
sometimes accompanied by fever and/or leukocytosis.
- Up to 43% of patients have at least one site of extranodal involvement (intracranial,
spine,
and head and neck),
which carries a worse prognosis.
Imaging findings:
- Imaging findings are often nonspecific,
overlapping with a variety of neoplastic and nonneoplastic conditions.
- Imaging studies are useful in evaluating multifocality and response to treatment.
- The final diagnosis is based on anatomopathological and immunohistochemical analysis.
Case Nº 4:
25-year-old woman with left exophthalmos.
Figure 7: Contrast-enhanced MRI.
A left solid expansive lesion is seen,
predominantly extraconal.
It is isointense on T1WI (A),
hyperintense on T2WI (C,D) and there is heterogeneous enhancement after gadolinium administration (B).
It is also evident a cephalic displacement of the ocular globe (C,D).
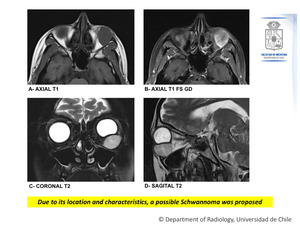
Fig. 7: Case Nº 4:
25-year-old woman with left exophthalmos.
Contrast enhanced MRI.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Biopsy result: RHABDOMYOSARCOMA
Generalities:
- Malignant neoplasm originated in primitive mesenchymal cells (pluripotential) that have the capacity to differentiate into skeletal muscle.
- It is the most common mesenchymal tumor in children.
- Corresponds approximately to 5% of all childhood cancers.
- Presentation: 70% occurs in children under 12 years of age.
- 35%–40% of rhabdomyosarcomas arise in the head and neck: Orbit,
parameningeal sites,
neck or face soft tissues and nasal cavity
- The orbital location has a better prognosis (80-90% disease-free survival)
- Parameningeal sites as middle ear,
paranasal sinus,
nasopharynx,
masticator space,
pterygopalatine fossa and parapharyngeal space,
have a worse prognosis (40-50% disease-free survival).
- Intracranial extension is seen in up to 55%
- In the orbit,
the origin can be primary or secondary (local spread or as a site of metastasis).
Clinical presentation: Aggressive,
rapidly growing tumor.
- Rapidly progressive proptosis.
- Globe displacement.
- Often conjunctival and palpebral swelling.
Imaging findings:
- Unilateral soft tissue mass.
- Mostly located in the extraconal compartment.
- Variable enhancement after contrast media administration.
- Usually has an aggressive behavior: Bone remodeling or destruction,
and soft tissue invasion.
CT scan is useful to evaluate bone involvement.
The mass is isoattenuated relative to muscle.
MRI is useful in better depicting the mass characteristics and detects intracranial extension.
- Isointense mass on T1WI and hyperintense to muscle and brain on T2WI.
- The globe is often displaced but rarely invaded.
- Meningeal enhancement can be seen in intracranial involvement.
Other considerations:
- Regional lymph node metastases are rare except in advanced disease.
- Metastases are hematogenous,
but orbital rhabdomyosarcoma is less likely to develop generalized metastatic disease.
Case Nº 5:
27-year-old man.
History of left ocular melanoma operated 3 years before.
Figure 8: Contrast-enhanced MRI.
There is a right solid intraconal mass that is slightly hyperintense with a hypointense capsule on T1WI (A),
hypointense on T2WI (B),
that shows homogeneous enhancement with gadolinium (C).
There is mass effect,
characterized by cephalad displacement of the optic nerve and caudal displacement of the inferior rectus muscle (B).
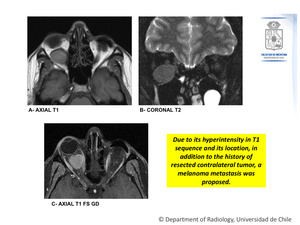
Fig. 8: Case Nº 5:
27-year-old man. History of left ocular melanoma operated 3 years before.
Contrast enhanced MRI.
References: Department of Radiology, Hospital Clínico Universidad de Chile, Universidad de Chile, 2018.
Biopsy result: MELANOMA METASTASIS
Generalities:
- Metastasis from other cancers constitute 1-13% of orbital tumors.
- The most frequent primary tumors are breast (48-53%),
prostate,
melanoma,
and lung.
- Some cancers have a predilection for specific locations in the orbit.
For example,
breast cancer tends to metastasize to orbital fat and muscle,
prostate cancer to bone,
and melanoma to muscle.
Clinical presentation:
The symptoms manifest quickly,
with progression occurring over weeks to months.
There may be proptosis and motility alterations.
Imaging appearance: Variable depending on the primary tumor.
In the particular case of melanoma metastasis,
melanin shows increased T1 signal intensity and decreased T2 signal intensity.
The degree of melanomatous pigmentation is variable and correlates with quantitative T1 signal:
- The higher the melanin content,
the higher the hyperintensity on T1WI,
the worse the prognosis.
- Up to 20% of melanomas are amelanotic,
thereby lacking characteristic MRI appearance.
