ECR 2019 / C-3544
Percutaneous CT-guided ablation of adrenal adenomas
Congress:
ECR 2019
Poster Number:
C-3544
Type:
Educational Exhibit
Keywords:
Ablation procedures, Percutaneous, CT, Interventional non-vascular, Abdomen, Endocrine disorders, Hypertension
Authors:
J. A. Torres de Abreu Macedo, N. Pereira da Silva, A. I. Aguiar, F. Alves, P. Donato; Coimbra/PT
DOI:
10.26044/ecr2019/C-3544

Fig. 1:
Women, 38 years.
Axial CT image obtained in prone position, shows...
.
Radiofrequency electrode extending into the aldosteronoma (B and C).
Axial CT image after termoablation (D).")
Fig. 2:
Men, 34 years.
Axial CT image obtained in prone position, shows aldosteronoma...

Fig. 3:
Men, 45 years old, with uncontrollable arterial hypertension.
Axial CT image...

Fig. 4:
Men, 48 years old, with uncontrollable arterial hypertension.
Axial CT image...

Fig. 5:
Women, 52 years old, with aldosteronoma.
Axial CT image obtained in prone...

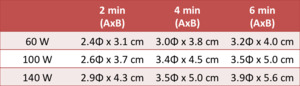
Fig. 6:
Adjustment of power and time according to lesion size.