ECR 2019 / C-3619
Pediatric cervical spine: Radiologic anatomy, normal variants and common pitfalls
Congress:
ECR 2019
Poster Number:
C-3619
Type:
Educational Exhibit
Keywords:
Trauma, Congenital, Diagnostic procedure, CT, Conventional radiography, Paediatric, Neuroradiology spine, Emergency
Authors:
M. M. M. Ashour1, S. Salah2, P. M. A. D. Mohamed Abouelhoda2, A. Mugahid2, M. A. Abou El Ela2, A. H. A. H. Ibrahim2; 1Cairo, New Cairo/EG, 2cairo/EG
DOI:
10.26044/ecr2019/C-3619
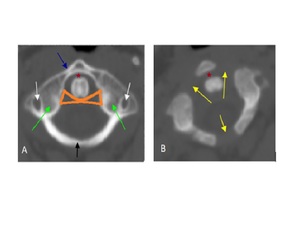
 and two posterior neural arches (red) which are ossified at birth separated by synchondrosis.")
Fig. 2:
The primary ossification centers of the atlas; one anterior arch (green) and...
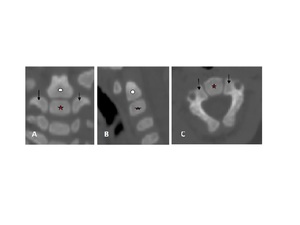
 coronal, (B) sagittal reformat and (C)axial view showing the primary ossification centers of the axis; one for the vertebral body (red Asterisk), one for each neural arch (arrow), and one for the dens (white circle).")
Fig. 3:
CT cervical spine (A) coronal, (B) sagittal reformat and (C)axial view showing...
 of 1.5-year-old child showing the normal expected appearance of the cervical spine ossification centers at that age with open subdental synchondrosis (black arrow), and neurocentral synchondrosis (red arrows), and (B) 6- year- old child showing the secondary ossification center at the tip of dens (red arrow), and fusion of the subdental synchondrosis with still visualized fusion line (green arrow).")
Fig. 4:
Coronal reformatted CT cervical images; (A) of 1.5-year-old child showing the...
 and two neural arches (red), separated by synchondrosis.")
Fig. 5:
The anatomy of the subaxial cervical vertebra; the body (yellow) and two neural...
, unfused ring apophysis can be mistaken for an avulsion but normal physeal plates can be recognizable by their smooth, regular structures with subchondral sclerotic lines.")
Fig. 6:
Reformatted CT Sagittal view of the cervical spine; superior and inferior ring...

Fig. 7:
The transverse bands of the cruciform ligament.
, apical ligament (red line), superior band of cruciate ligament (white arrow), tectorial membrane (blue arrow) and posterior atlanto- occipital membrane (yellow arrow).")
Fig. 8:
Sagittal reformatted CT cervical spine illustrates various ligaments of the...
 lateral, and (B) AP cervical radiography of adequate criteria.")
Fig. 9:
(A) lateral, and (B) AP cervical radiography of adequate criteria.

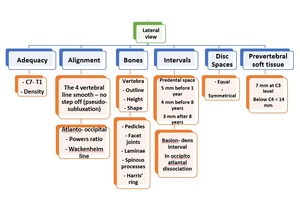
Fig. 10:
Checklist for reporting lateral cervical x- ray.
, the posterior vertebral line (green line), the spinolaminar line (yellow line) and the pre- vertebral line (orange line).")
Fig. 11:
Cervical X- ray sagittal view showing the anterior vertebral line (black line),...

Fig. 12:
Sagittal view cervical spine shows Harris ring which is distinct ring on...
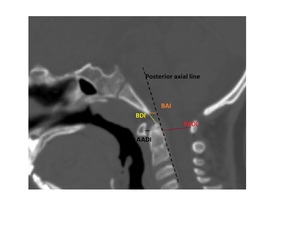
, anterior atlanto-dental interval (AADI), posterior atlanto-dental interval (PADI) and basion- atlanto interval (BAI) which is measured in-between the basion to the posterior axial line which is a line tangential to the posterior surface of C2.")
Fig. 13:
CT cervical spine, midsagittal of normal patient illustrates, the basion-dens...

Fig. 14:
Craniometric lines

Fig. 15:
The Wackenheims line illustrated on lateral x- ray cervical spine by...

Fig. 16:
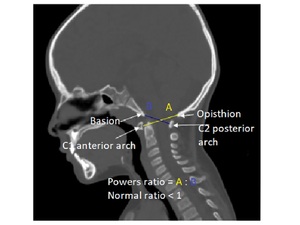
How to calculate Powers ratio.

Fig. 17:
Checklist for reporting AP view cervical x- ray.
 cervical x- ray")
Fig. 18:
Checklist for Open mouth (Odontoid view) cervical x- ray
, with no abnormal prevertebral soft tissue thickening (green arrow), in prescence of pseudosubluxation the anterior aspect of the posterior arch of C2 vertebra should be within 1-2 mm of the Swischuck line/ posterior cervical line (black line) that is drawn between the anterior aspect of the posterior arch of C1 (red arrow), to the anterior aspect of the posterior arch of C2 (white arrow); deviation by more than 2 mm is indicative of true subluxation (this line is only applied in presence of anterior diplacement).")
Fig. 19:
Cervical x-ray sagittal view showing mild anterior displacement of C2 over C3...

Fig. 20:
Sagittal CT at the cranio- cervical junction illustrates f between the anterior...

Fig. 21:
C1 posterior arch anomalies

Fig. 22:
CT axial view at the level of the atlas vertebra; showing posterior arch defect...

Fig. 23:
Odontoid anomalies

Fig. 24:
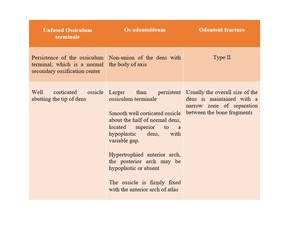
Differential diagnosis for ossific density cranial to the dens.
, appearnace of the ossiculum terminale (white), unfused basilar synchondrosis (black) and anterior wedging of C3 vertebral body (orange).")
Fig. 25:
Sagittal reformated cervical CT showing prevertebral soft tissue widening...

Fig. 26:
Odontoid aplasia

Fig. 27:
Graph illustrating the three types of atlas fractures.