ECR 2019 / C-3659
Necrotizing Pneumonia: a rare yet important pathology.
Congress:
ECR 2019
Poster Number:
C-3659
Type:
Educational Exhibit
Keywords:
Pathology, Infection, Diagnostic procedure, CT-High Resolution, CT-Angiography, CT, Thorax, Lung
Authors:
M. Valle Franco1, L. Martínez González1, J. de la Calle Lorenzo2, C. Torrez Villarroel2, M. Berlioz Ortiz1, I. M. LÓPEZ GARCÍA1, F. J. SOMALO ALFARO2, A. Pérez Termenón1, M. Pérez Rodríguez1; 1León/ES, 2León, Castilla y León /ES
DOI:
10.26044/ecr2019/C-3659

Fig. 1

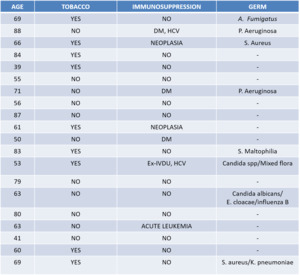
Table 1

Fig. 2

Fig. 3

Fig. 4:
A: Chest x-ray. B: Contrast-enhanced chest CT. Consolidation in the right upper...

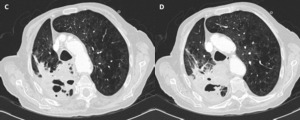
Fig. 5:
C-D: Contrast-enhanced chest CT. Great centrilobular emphysema and...

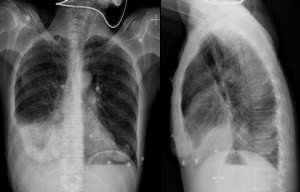
Fig. 6:
PA and lateral chest x-ray: Right pleural effusion.

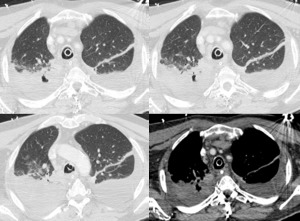
Fig. 7:
Contrast-enhanced chest CT: Consolidation in the middle lobe with an air cavity...

Fig. 8:
PA and lateral chest x-ray: Consolidations in the right lung.

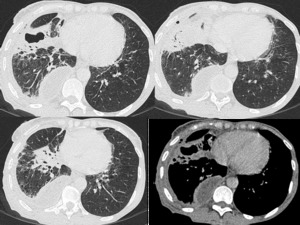
Fig. 9:
Contrast-enhanced chest CT: Bilateral pleural effusion and consolidation in the...