ECR 2019 / C-3664
Serous borderline ovarian tumors: tips, tricks and mimics on magnetic resonance imaging
Congress:
ECR 2019
Poster Number:
C-3664
Type:
Educational Exhibit
Keywords:
Genital / Reproductive system female, Oncology, MR, MR-Diffusion/Perfusion, Diagnostic procedure, Multidisciplinary cancer care
Authors:
H. Sahin, Y. Pekcevik; Izmir/TR
DOI:
10.26044/ecr2019/C-3664

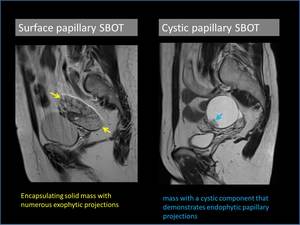
Fig. 2:
Examples of surface and cystic papillary subtypes of serous borderline ovarian...

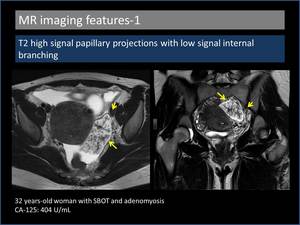
Fig. 3:
T2 high signal papillary projections with low signal internal branching

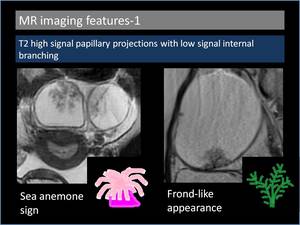
Fig. 4:
Sea anemone sign and frond-like appearance in serous borderline ovarian tumours.

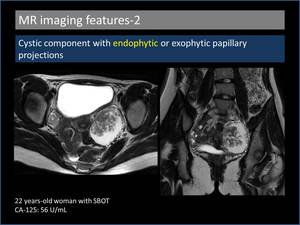
Fig. 5:
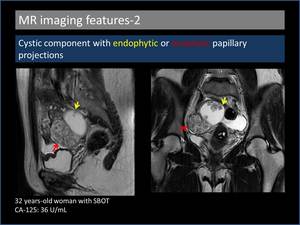
Cystic component with endophytic papillary projections.

Fig. 6:
Cystic component with endophytic and exophytic papillary projections.

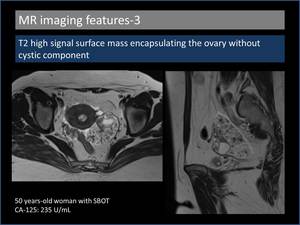
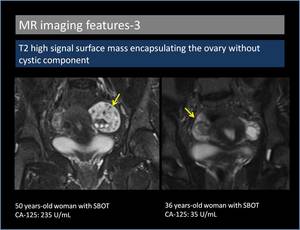
Fig. 7:
T2 high signal surface mass encapsulating the ovary without cystic component.

Fig. 8:
T2 high signal surface mass encapsulating the ovary without cystic component.

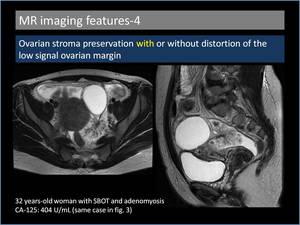
Fig. 9:
Ovarian stroma preservation with distortion of the low signal ovarian margin.

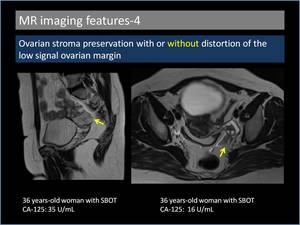
Fig. 10:
Ovarian stroma preservation without distortion of the low signal ovarian margin

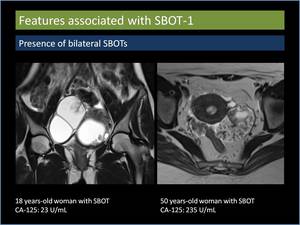
Fig. 11:
Presence of bilateral serous borderline ovarian tumours.

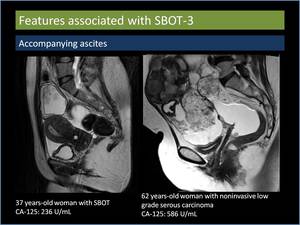
Fig. 13:
Accompanying ascites.

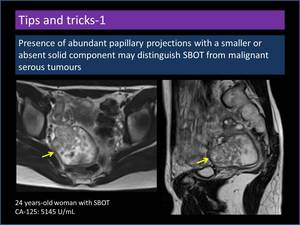
Fig. 14:
Presence of abundant papillary projections with a smaller or absent solid...

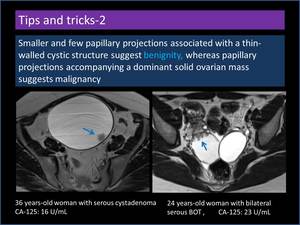
Fig. 15:
Smaller and few papillary projections associated with a thin-walled cyst

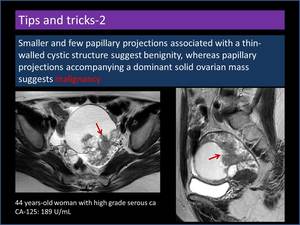
Fig. 16:
Papillary projections accompanying a dominant solid ovarian mass.

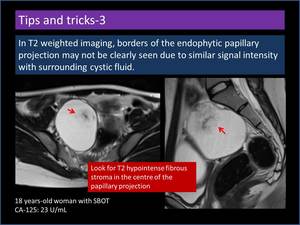
Fig. 17:
Endophytic papillary projection with subtle borders.

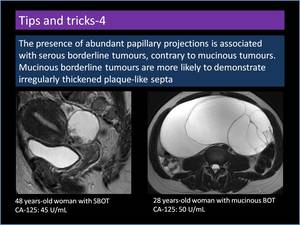
Fig. 18:
Difference between serous and mucinous borderline tumours.

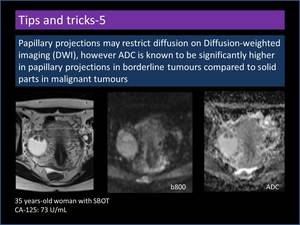
Fig. 19:
Diffusion-weighted imaging features of papillary projections.

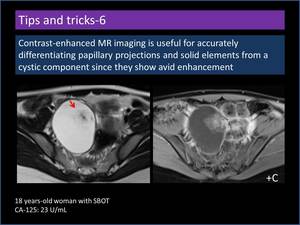
Fig. 20:
Contrast-enhanced MR imaging features of papillary projections.