TAVR (Transcatheter aortic valve replacement) is a therapeutic alternative to conventional surgery,
which consists of the placement of an aortic valve bioprosthesis,
which replaces the native valve displacing it against the aortic wall in the deployment.
There are two main approaches for the implantation of the prosthesis:
-Peripherally: trans-femoral and subclavian.
-Transapical route (through the apex of the left ventricle),
which is used in cases in which the former is contraindicated.
Whatever the path of choice is necessary to know the anatomy of the cardiac valvular apparatus,
ascending,
descending aorta and peripheral arteries for proper placement,
all these measures,
will be definitive to individualize the prosthesis to place,
decide the most appropriate approach and,
in some cases,
even contraindicate the percutaneous procedure.
ROLE OF THE ANGIOTOMOGRAPHY AND OBTAINING THE IMAGES
Aortic studies of non-synchronized CT often show artifacts at the origin of the aorta.
The study protocol ideally used is similar to that performed for a coronary CT angiography,
using a multislice CT.
A simple CT without contrast is performed to assess coronary and aortic calcium levels with an adequate cardiac synchronization (previous preparation).
Subsequently,
CT angiography study with ROI in ascending aorta using 80-100 ml of EV contrast,
by retrospective analysis of the images.
The study of cardiac CT requires the acquisition in synchronized form with the cardiac rhythm,
to avoid the artifacts of movement produced by the normal beat of the heart and so that the images can be reconstructed at any moment of the most appropriate cardiac phase or heart.
ROLE OF THE REPORT
An adequate report for TAVR must have information,
clear and accurate,
so the report must be complete for the cardiologist or interventional physician requesting the study.
The anatomical regions to be measured for the report can be classified according to their usefulness in the following way:
Measures to define the prosthesis to implant: Anatomy of the Aortic valve which must be performed in the systolic phase since it's the moment of maximum valve opening measuring:
- Area of the aortic ring.
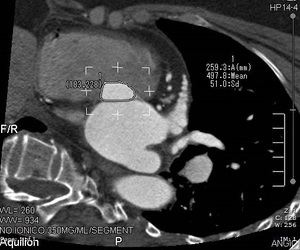
Fig. 3: CT image in which measurement of the area of the aortic annulus is observed.
- Perimeter of the aortic ring.
- Diameter in major axis.

Fig. 5: CT image in which measurement of all areas of the aortic ring is observed.

Fig. 6:
CT image in which measurement of all the areas of the aortic ring is observed, important calcifications are observed at the level of the leaflets, which must be reported in the report.
- Diameter on short axis.

Fig. 4: CT image in which a greater and smaller area measurement of the aortic ring is observed.
- Average diameter.
- Average diameter from the area.
- Average diameter from the perimeter.
- Distance from the annular plane to the right and left coronary ostium.
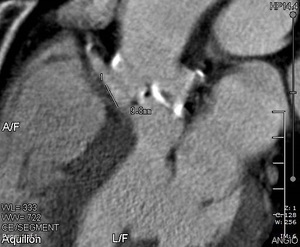
Fig. 8: CT image that shows the distance from the annular plane to the right coronary ostium.

Fig. 9:
CT image that shows the distance from the annular plane to the left coronary ostium
- Minimum diameter of the ascending aorta at the level of the sino-tubular junction.

Fig. 10:
CT image showing the minimum diameter of the ascending aorta at the level of the sino-tubular junction.
- Maximum diameter of the ascending aorta and distance to the aortic annulus.
Measures to define surgical access:
- Aorto-ventricular angle.
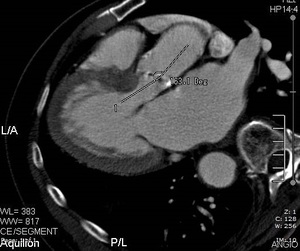
Fig. 11: CT image showing measurement of the aorto-ventricular angle.

Fig. 12:
CT image showing measurement of the aorto-ventricular angle.
- Minimum diameter of the left ventricle outflow tract.

Fig. 14:
CT image showing minimum left ventricular outflow tract diameter.
- Anterior and posterior diameter at the exit of the brachiocephalic trunk and the distance of the aortic ring.
- Measurement of the abdominal aorta in its transverse diameter.
- Measurement of the right and left common iliac artery.

Fig. 13:
CT image showing the measurement of the left common femoral artery.
- Measurement of the right and left external iliac artery
Cardiac anatomy.
- Distribution of coronary arteries.
- Cardiac dominance.
- Origin of coronary arteries with respect to coronary sinuses.
