-Lipoma arborescence
Pathology and clinical presentation:
Lipoma arborescens is a benign joint disease in which non-neoplastic deposits replace and distend the synovium (8).
It is characterized by villous proliferation of the synovium,
with the replacement of the sub-synovial connective tissue by mature fat cells (7).
Its etiology and pathogenesis are still unknown (7).
Lipoma arborescens is most commonly located at the suprapatellar pouch and patients usually complain of painless swelling of the knee joint along with joint effusion (Fig. 1); however the limited range of motion is not frequently reported (7).
Imaging features:
X-ray usually shows the fullness of the suprapatellar pouch associated with some fat lucencies.
A complementary Ultrasound scan is usually done and typically shows frond-like villous projections of the synovium with joint effusion (10) (Fig. 2).
MRI shows large frond-like mass arising from the synovium,
with signal intensity similar to fat on all pulse sequences.
Moreover,
the synovial lining and synovial fluid may enhance in post-contrast studies (7) (Fig. 3).
Radiological appearance with representative case:
Radiograph:

Fig. 1: Knee radiography lateral view demonstrates homogeneous soft tissue opacity within the suprapatellar recess displacing the quadriceps tendon
with radiolucencies representing fatty infiltration of the synovium.
Ultrasound:

Fig. 2: Ultrasound of the knee joint shows moderate to severe joint effusion with low-level internal echoes and evident frond like synovial thickening in the supra-patellar recess.
MRI:

Fig. 3: (A) T1 weighted MR image of the knee joint demonstrating multiple inter-articular frond-like projections in a background of marked joint space effusion.(B) T1 fat sat weighted MR image shows complete fat suppression of the synovial thickening.(C) T1 Fat Sat weighted MR image post contrast injection showing mainly peripheral enhancement.
Treatment:
Recommended treatment is open synovectomy (7).
Differential diagnosis:
*Synovitis: shows joint effusion along will synovial thickening and enhancement in the absence of fatty infiltration.
*Pigmented Villonodular Synovitis: shows low signal and blooming artifacts in the MR gradient echo sequence due to hemosiderin deposition (Fig. 6).
Erosive changes may present in advanced cases.
(Fig. 8)
-Pigmented Villonodular Synovitis
Pathology and clinical presentation:
PVNS represents a benign,
hypertrophic synovial process characterized by villous,
nodular,
and villonodular proliferation and pigmentation from hemosiderin (4).
It presents either in a localized form,
with minimal rates of recurrence after surgical resection,
or in a diffuse form (Fig. 7),
with an expansive growth pattern showing the formation of osseous erosions and extra-articular manifestation.
The etiology of PVNS has been attributed to either an inflammatory process; repeated hemorrhage into the joint,
an occult synovial hemangioma or repetitive mild trauma; neoplasia; or a disorder of lipid metabolism (4).
Discomfort is always present but the clinical presentation is variable (5).
Imaging features:
PVNS usually manifests as a nonspecific joint effusion on radiographs,
although occasionally the fluid may appear dense,
a finding suggestive of hemorrhagic effusion (11) (Fig. 4).
Bone erosions can be seen in 25% of cases (Fig. 8)
MRI reveals a lobulated mass with reduced signal intensity on T1 and T2 weighted images due to hemosiderin (10).
Blooming artifact on GRE images is characteristic (11) (Fig. 6 ).
Radiological appearance:
Radiograph:
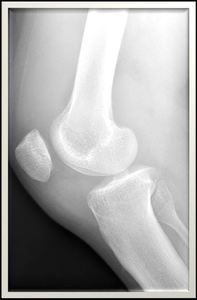
Fig. 4: Knee radiograph, lateral view showing obliteration and fullness of the supra-patellar recess,Hoffa's fat pad and posterior aspect of the knee joint. No bony erosive changes detected.
Ultrasound:
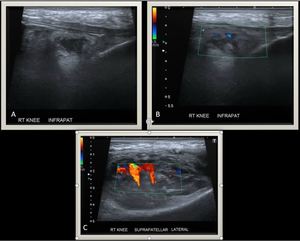
Fig. 5: Knee Ultrasound reveals a large heterogeneous soft tissue mass with internal vascularity on color Doppler flow having supra (C) and infra patellar extension (A) and (B).
MRI:
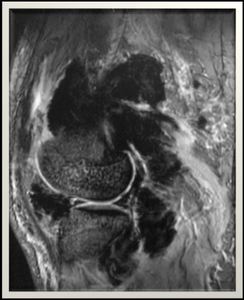
Fig. 6: Knee MR gradient echo sequence, lateral view demonstrates multiple irregular intra and extra articular synovial soft tissue masses with
evidence of marked blooming artifacts.
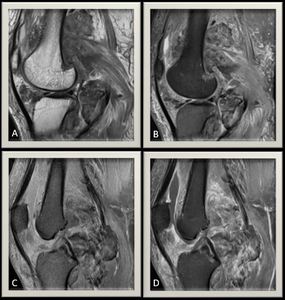
Fig. 7: (A) Proton density MR image and (B) Proton density MR images with fat suppression ,sagital view of the knee joint illustrating multiple heterogeneous multilobulated intra and extra-articular masses mainly occupying the posterior aspect of the knee joint. (C) T1 Fat Sat weighted MR image and (D) Post contrast sequence demonstrating heterogeneous enhancement of the masses with evident joint effusion with enhancing synovium denoting synovitis.
-Another example case of a different patient :
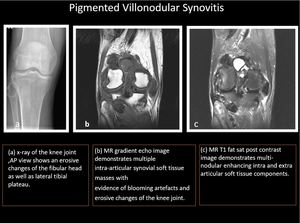
Fig. 8: Another case of Pigmented villonodular synovitis demonstrating erosive changes of the fibular head as seen in the radiograph (A).
Treatment:
The treatment options for diffuse intraarticular PVNS have been limited to surgery and irradiation until recently (4).
Differential diagnosis:
*Synovial chondromatosis: Blooming artifacts are uncommon.
*Lipoma arborescence: (Fig. 3) demonstrates frond-like projections of synovial fatty infiltration.
Blooming artifacts are uncommon.
-Hemophilic arthropathy
Pathology and clinical presentation:
Hemophilia is an inherited bleeding disorder due to deficiency of factor VIII (hemophilia A) or factor IX (hemophilia B) resulting in insufficient thrombin generation leading to recurrent intra-articular hemorrhages (hemarthroses).
The knee is most frequently affected by hemophilic arthropathy.
Chondrocytes apoptosis (cartilage degeneration) and synovial hypertrophy (synovitis) as a result of recurrent hemarthrosis contribute to the core pathogenesis of hemophilic arthropathy (1).
Symptoms include joint swelling,
warmth (with or without painful symptoms) and reductions in the motion of the knee (1).
Imaging features:
Joint changes in radiographs include in order of severity; soft tissue swelling,
osteoporosis,
overgrowth of the epiphysis,
subchondral bones cysts,
squaring of the patella,
joint space narrowing and loss of cartilage (13) (Fig. 9).
The classical features on MR include synovial hypertrophy and hemosiderin deposition.
Blooming artifact from hemosiderin on GRE images obscures underlying synovium (Fig. 10).
Radiological appearance:
Radiograph:

Fig. 9: Left knee radiograph shows reduced bone density with multiple
subchondral cystic changes. Widening of the intercondylar notch is noted as
well.
MRI:
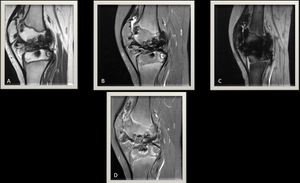
Fig. 10: (A) T1 weighted MR image of the knee joint and (B) T2 fat sat weighted MR image demonstrating synovial thickening with multiple inter-articular low signal intensities and associated articular cartilage loss with erosive changes.(C) MR gradient echo image, lateral view illustrating marked blooming artifacts due to hemosiderin deposition.
(D) T1 Fat sat post contrast study showing synovial enhancement in keeping with synovitis.
Treatment:
The only treatment is done mainly to stop recurrent bleeding by primary prophylaxis replacing the deficient clotting factor which must begin early in life.
Once developed,
HA can be addressed with basic surgical procedures including radiosynovectomy (RS),
chemical synovectomy (CS),
arthroscopic synovectomy (AS),
arthroscopic joint debridement and total knee arthroplasty (TKA) (1).
Differential diagnosis:
*Pigmented Villonodular Synovitis: shows low signal and marked blooming artifacts in MR gradient echo sequence due to hemosiderin deposition Fig. 6.
Age of the patient and clinical history can guide to the definite diagnosis of hemophilic arthropathy.
*Synovial chondromatosis: Marked blooming artifacts are not common.
-Synovial chondromatosis
Pathology and clinical presentation:
Synovial chondromatosis has been divided into primary and secondary forms.
Primary synovial chondromatosis represents chondroid metaplasia in the synovium of a joint with resultant formation of multiple intraarticular chondral bodies while Secondary synovial chondromatosis is associated with joint abnormalities,
such as mechanical or arthritic conditions,
that cause intraarticular chondral bodies (6).
Clinical symptoms typically include pain,
swelling,
and restriction of range of motion (6).
Imaging features:
Radiographs reveal multiple intraarticular calcifications in 70%–95% of cases of primary synovial chondromatosis which are usually innumerable and very similar in shape,
in contrast to secondary chondromatosis in which the calcifications are fewer in number and variable in size.
Fragments of primary chondromatosis may progress to further maturation and enchondral ossification with a peripheral rim of the cortex and inner trabecular bone.
A target appearance may also be seen,
consisting of a central focus and a single rim of calcification (6).
The MR imaging appearance of primary synovial chondromatosis intraarticular signal intensity similar to that of muscle on T1-weighted images,
with high signal intensity on T2-weighted images and focal areas of low signal intensity with all pulse sequences. The areas of signal void corresponded to regions of calcification on radiographs or CT scans and became more conspicuous on gradient-echo MR images owing to magnetic susceptibility effects (6).
Radiological appearance:
Radiograph and MRI:
An example case of intra-articular ossified loose bodies representing primary osteochondromatosis.
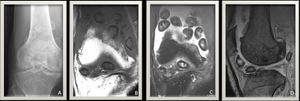
Fig. 12: (A) Knee radiograph AP view demonstrates intra-articular ossified loose bodies surrounding the joint lines. No erosive changes detected.
(B) T1 weighted MR image of the knee joint and (C) T2 weighted MR image with fat suppression show multiple intra-articular low signal intensities of relatively similar size following the bone signal intensity. (D) MR gradient echo image shows no appreciable blooming artifacts.
Treatment:
Surgical resection is the treatment of choice with recurrence rate from 3 to 23 % (6).
Differential diagnosis:
*Pigmented Villonodular Synovitis: shows low signal and marked blooming artifacts in MR gradient echo sequence due to hemosiderin deposition (Fig. 6)
*Lipoma arborescence: (Fig. 3) demonstrates frond-like projections of synovial fatty infiltration.
Blooming artifacts are uncommon.
-Synovial hemangioma
Pathology and clinical presentation:
Synovial hemangiomas are rare intra-articular tumors of the knee in children and young adults who are often diagnosed late (2).
There is usually a history of recurrent atraumatic painless bloody effusions.
They can be focal or diffuse in their involvement of the joint (3).
Clinical presentation often includes pain,
joint swelling,
and recurrent joint effusions,
with or without limitation in range of motion (3).
Imaging features:
Plain radiographs are not diagnostic in half of the patients and could show effusion and soft tissue masses (Fig. 13).
A periosteal reaction,
phleboliths,
and bone erosions are also identified with plain radiographs (14).
Ultrasonographic examinations show the vascular structures within the lesion (14) (Fig. 14).
MRI: Synovial hemangiomas appear as intermediate signal intensity on T1-weighted images,
isointense or slightly hyperintense than surrounding muscles.
The lesion appears hyperintense on T2-weighted and fat-suppressed images.
Thin,
serpentine and low-intensity septa are also detected on T2-weighted and fat-suppressed images.
After contrast administration,
the lesion shows marked enhancement (14) (Fig. 15).
Radiological appearance:
Radiograph:

Fig. 13: Knee radiograph lateral view shows no definite bone or soft tissue pathology.
Ultrasound:
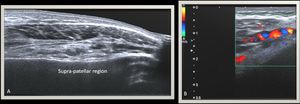
Fig. 14: Ultrasound of the knee joint showing heterogeneous multilobular mass with internal vascularity seen occupying the supra-patellar recess.
MRI:

Fig. 15: Knee joint MRI T2WI (A), T2WI FS (B) show a supra-patellar tortuous lace-like mass lesion of intermediate signal on T1WI and high signal on fluid-sensitive sequences; post-contrast study (D) shows intense enhancement with internal tortuous vascular channels that could be tracked to genicular branches of the popliteal artery(F).(E) Gradient echo sequence showing no significant blooming artifacts.
Treatment:
Treatment generally involves open or arthroscopic surgical excision of the entire hemangioma,
with partial or total synovectomy (3).
Open excision is necessary for large lesions which have infiltration into surrounding muscles (2).
Differential diagnosis:
*Pigmented Villonodular Synovitis: shows low signal and marked blooming artifacts in the MR gradient echo sequence due to hemosiderin deposition (Fig. 6).
*Synovial chondromatosis: Absent intense enhancement.
-Septic arthritis
Pathology and clinical presentation:
Septic arthritis may develop as a result of hematogenous seeding,
direct introduction,
or extension from a contagious focus of infection (19).
Delayed diagnosis may result in cartilage and joint destruction arising from the action of enzymes released from neutrophils,
synovial cells,
and bacteria (15).
Septic arthritis typically presents as a hot,
swollen,
tender joint with a reduced range of movement (16).
Imaging features:
Plain radiograph findings are non-specific for joint effusion,
especially in the suprapatellar pouch (Fig. 16).
Thickened enhancing synovium with peri-synovial edema on a background of joint effusion are the main characteristic features on MRI imaging (Fig. 17) (15).
Radiological appearance:
Radiograph:

Fig. 16: Knee radiograph, AP and lateral views demonstrate a marked soft tissue swelling about the anterior and lateral aspects of the knee joint line.No definite erosive changes.No periosteal reaction.
MRI:

Fig. 17: Knee MR T1WI FS C+ (A),(B),axial and sagital views respectively reveal knee joint effusion distending the supra-patellar recess and demonstrates peripherally enhanced thickened synovium. Few internal plica/ septa are seen in the effusion.(C),(D) Post-contrast MR images ,axial and sagital views respectively showing subcutaneous small abscess formation lateral to the patella. A deeper sinus track is seen leading towards the joint (Blue arrows).
Treatment:
Antibiotics together with removal of any purulent material are the mainstay of treatment (16).
Differential diagnosis:
*Reactive or inflammatory synovitis attributed to other different systemic diseases like R.A.
*Lipoma arborescence: (Fig. 3) demonstrates frond-like projections of synovial fatty infiltration.
Blooming artifacts are uncommon.
-Rheumatoid Arthritis
Pathology and clinical presentation:
Rheumatoid arthritis is a chronic systemic autoimmune disorder that primarily affects the synovium and if left untreated leads to disorganization and destruction of the joints.
Joint destruction results in severe deformity and disability (17).
Synovial hypertrophy and angioneogenesis develop in the chronic phase of the condition,
the hypertrophied synovium becoming locally invasive at the synovium-cartilage interface where it is thought to be responsible for causing bone erosions and subsequent joint destruction (17).
Patients most frequently present with pain and stiffness,
Involvement is usually bilateral and symmetric (17).
Imaging features:
Radiographs show soft-tissue swelling,
periarticular osteopenia,
joint space loss,
joint subluxation and marginal erosions (17) (Fig. 18).
MRI is the best modality in detecting synovial hypertrophy,
inflammation,
thickening,
and enhancement (Fig. 19) (Fig. 20).
Radiological appearance:
Radiograph:

Fig. 18: Knee X-ray AP and lateral views demonstrates asymmetrical osteodegenerative changes of the knee joint mainly involving the lateral compartment. Fullness of the supra-patellar recess noted denoting joint effusion. Mild reduction of the bone density seen.
MRI:
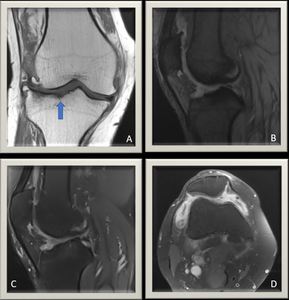
Fig. 19: Knee joint MRI T1WI coronal view(A) demonstrates again the osteo-degenerative changes with evident cortical erosive changes of the tibial plateau (Blue arrow). (B) Gradient echo MR image shows no evidence of blooming artifacts. (C) Proton density MR image with fat suppression illustrating thickened synovium with moderate joint effusion.(D) T1WI FS C+ axial view shows enhanced thickened synovium/synovitis.
Another example case of rheumatoid arthritis patient:
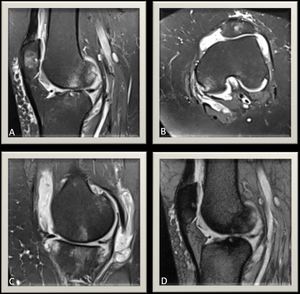
Fig. 20: Another case of rheumatoid arthritis: Knee MRI PDFS(A),(B) sagital and axial views respectively illustrates osteoarthritic changes with evident tri-compartmental sub-articular marrow edematous and cyst-like changes and focal patchy subchondral marrow edema changes. MR PDFS MR image at different level (C)illustrates thickened synovium with moderate-severe knee joint effusion.Gradient echo MR image,sagital view (D) shows no evidence of blooming artifacts.
Treatment:
Treatment consists of two main pillars.
Disease-modifying antirheumatic drugs are the only class of drugs that have an influence on the course of the disease (18).
Physical therapy is the other pillar of treatment to preserve joint function (18).
Differential diagnosis:
*Septic arthritis: Clinical history,
laboratory results correlation,
and diagnostic tapping can help to reach the diagnosis.
*Reactive or inflammatory synovitis.



 T1 weighted MR image of the knee joint demonstrating multiple inter-articular frond-like projections in a background of marked joint space effusion.(B) T1 fat sat weighted MR image shows complete fat suppression of the synovial thickening.(C) T1 Fat Sat weighted MR image post contrast injection showing mainly peripheral enhancement.")

 and infra patellar extension (A) and (B).")

 Proton density MR image and (B) Proton density MR images with fat suppression ,sagital view of the knee joint illustrating multiple heterogeneous multilobulated intra and extra-articular masses mainly occupying the posterior aspect of the knee joint. (C) T1 Fat Sat weighted MR image and (D) Post contrast sequence demonstrating heterogeneous enhancement of the masses with evident joint effusion with enhancing synovium denoting synovitis.")
.")

 T1 weighted MR image of the knee joint and (B) T2 fat sat weighted MR image demonstrating synovial thickening with multiple inter-articular low signal intensities and associated articular cartilage loss with erosive changes.(C) MR gradient echo image, lateral view illustrating marked blooming artifacts due to hemosiderin deposition.
(D) T1 Fat sat post contrast study showing synovial enhancement in keeping with synovitis.")
 Knee radiograph lateral view shows no definite soft tissue or bone pathology.
(B) T1 weighted MR image of the knee joint demonstrates two intra-articular low signal intensities of relatively similar size ( Blue arrows) representing the non-ossified intra-articular bodies.(C) PD MR image with fat suppression showing intermediate to high signal intensity of the lesions.")
 Knee radiograph AP view demonstrates intra-articular ossified loose bodies surrounding the joint lines. No erosive changes detected.
(B) T1 weighted MR image of the knee joint and (C) T2 weighted MR image with fat suppression show multiple intra-articular low signal intensities of relatively similar size following the bone signal intensity. (D) MR gradient echo image shows no appreciable blooming artifacts.")


, T2WI FS (B) show a supra-patellar tortuous lace-like mass lesion of intermediate signal on T1WI and high signal on fluid-sensitive sequences; post-contrast study (D) shows intense enhancement with internal tortuous vascular channels that could be tracked to genicular branches of the popliteal artery(F).(E) Gradient echo sequence showing no significant blooming artifacts.")

,(B),axial and sagital views respectively reveal knee joint effusion distending the supra-patellar recess and demonstrates peripherally enhanced thickened synovium. Few internal plica/ septa are seen in the effusion.(C),(D) Post-contrast MR images ,axial and sagital views respectively showing subcutaneous small abscess formation lateral to the patella. A deeper sinus track is seen leading towards the joint (Blue arrows).")

 demonstrates again the osteo-degenerative changes with evident cortical erosive changes of the tibial plateau (Blue arrow). (B) Gradient echo MR image shows no evidence of blooming artifacts. (C) Proton density MR image with fat suppression illustrating thickened synovium with moderate joint effusion.(D) T1WI FS C+ axial view shows enhanced thickened synovium/synovitis.")
,(B) sagital and axial views respectively illustrates osteoarthritic changes with evident tri-compartmental sub-articular marrow edematous and cyst-like changes and focal patchy subchondral marrow edema changes. MR PDFS MR image at different level (C)illustrates thickened synovium with moderate-severe knee joint effusion.Gradient echo MR image,sagital view (D) shows no evidence of blooming artifacts.")