The first part of the study was to validate the PSD mapping of the dose management system DOSE that is used at the Radiology Department of the University Hospitals Leuven.
Peak skin dose calculation in DOSE is an advanced tool that starts from the automatically received Radiation Dose Structured Report (RDSR) of the interventional procedure and uses the dosimetric and geometric parameters of each irradiation event in order to build the skin dose distribution map of the whole procedure.
Other affecting factors like the backscatter factor depending on field size,
spectrum and thickness,
the f-factor and the table and pad transmission factors are also included,
as suggested in the literature [6].
When it comes to the selection of the phantom,
this depends on the age of the patient and in addition,
if information on the weight and height of the patient exists,
then the system does not just use the standard adult or pediatric phantom,
but scales it to match the correct dimensions and provide a more patient-specific approach.
The validation of the aforementioned PSD tool was performed with experimental measurements on an Axiom Artis system (Siemens,
Germany) that is installed at the University Hospitals Leuven,
Campus Gasthuisberg.
For the measurements,
two phantoms,
one for adult and one for pediatrics,
were utilized.
Initially,
an elliptical phantom to mimic the trunk of the adult patient was designed ( Fig. 1 ).
The phantom is made of Plexiglas and consists of 10 plates of 3 cm thickness each,
which gives it a total length of 30 cm.
The width and heigth of the phantom are 40cm and 20cm respectively,
in accordance with the MIRD phantom (trunk including arms)[7].
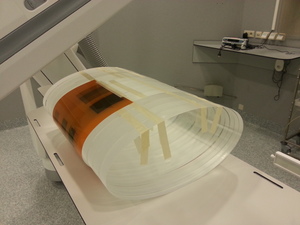
Fig. 1: Positioning of the elliptical phantom consisting of 10 Plexiglas plates of 3 cm each on the interventional table to mimic the patient’s trunk. Two Gafchromic films were wrapped around the phantom, covering the posterior – right – half anterior sides. This way, visualization of irradiations with different angulation and table positioning could be evaluated.
References: Qaelum NV - Leuven/BE
For the case of pediatric patients,
an anthropomorphic 10yo pediatric phantom (CIRS,
USA and provided by SCK-CEN,
Belgium) was utilized for the validation of the PSD map ( Fig. 2 ).
It has to be noted that this phantom does not include arms which can cause small discrepancies against the PSD tool of DOSE,
as in the calculation of DOSE,
arms are considered attached to the body.

Fig. 2: Positioning of the 10yo CIRS phantom (provided by SCK-CEN) on the interventional table to mimic the pediatric 10yo patient (the phantom does not include arms). The film was taped on the trunk of the phantom and covers the posterior – right – small part of the anterior sides.
References: Qaelum NV - Leuven/BE
Additionally,
XR-QA2 Gafchromic films of size 10 x 12 inch (~25 x 30 cm),
were used to validate the performance of the DOSE skin dose mapping in terms of the irradiated area on the two phantoms for a series of well-defined exposures with different table height,
positioning and tube angulation.
Additionally,
a Piranha dosimeter with the TO20 doseprobe was used during the measurements.
The dosimeter was not used for absolute dosimetry but for an overall evaluation,
as the PSD calculation of DOSE uses the Air Kerma at Reference Point as a starting point,
for every irradiation event that is included in the RDSR of the procedure.
Therefore,
this value is considered to have been validated during the Quality Assurance of the device.
After the completion of the measurements,
the reports were automatically sent through PACS to DOSE where we could directly compare the calculated skin dose map and the peak skin dose value against our validation experiments.
In the second part of the study,
four pediatric interventional cardiology cases from the hospital were evaluated.
The patients covered a wide range of age groups (4w-3.9kg,
9yo-36kg-136cm,
12yo-43kg-152cm,
15yo-75kg-175cm).
Qaelum’s DOSE platform provided the peak skin dose map for the correct dimensions of the pediatric patients.
For the intentions of this study,
we performed a second calculation for each case,
using the RDSR of the procedure and the standard adult phantom instead.
The use of the size-corrected versus the standard adult approach was then evaluated.
The third and last part of the project included “what if” scenarios for evaluating the effect of the correct phantom size under different irradiation techniques.
The adult,
10 yo and newborn standard phantoms were considered to undergo two procedures with the same three irradiation events focusing on the left side of the patient.
The only difference between the two procedures was that the table was moved 6cm between the events in the first procedure,
while in the second it was moved 5cm.
The effect on the PSD maps was then evaluated.


 on the interventional table to mimic the pediatric 10yo patient (the phantom does not include arms). The film was taped on the trunk of the phantom and covers the posterior – right – small part of the anterior sides. References: Qaelum NV - Leuven/BE")