ECR 2020 / C-01082
Techniques and disease patterns in paediatric small bowel MRI
Congress:
ECR 2020
Poster Number:
C-01082
Type:
Educational Exhibit
Keywords:
Paediatric, Colon, Small bowel, MR-Enterography, Contrast agent-oral, Imaging sequences, Technical aspects, Dilatation, Fistula, Inflammation, Not applicable, Observational, Performed at one institution
Authors:
S. McGurk, A. Kirby, A. J. Quigley, K. Kind; Edinburgh/UK
DOI:
10.26044/ecr2020/C-01082

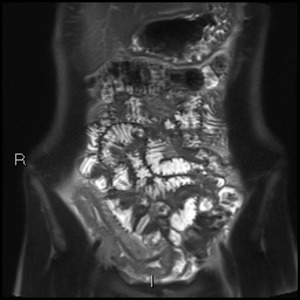
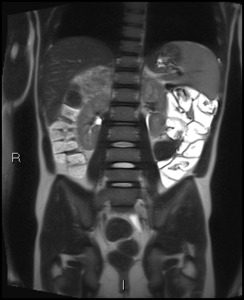
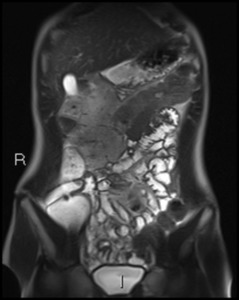
Fig. 1:
Coronal T2 HASTE showing thickened, T2 hyperintense ileum with deep ulceration...

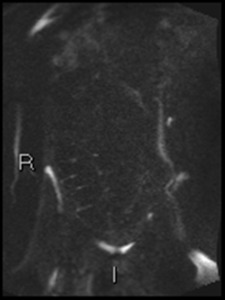
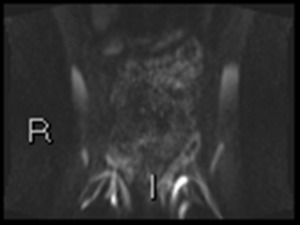
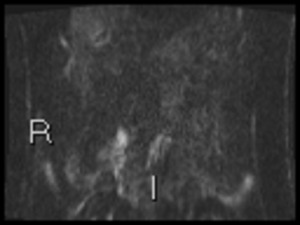
Fig. 4:
Axial DWI b1300. Fluid signal is suppressed. Remaining high signal, seen as...

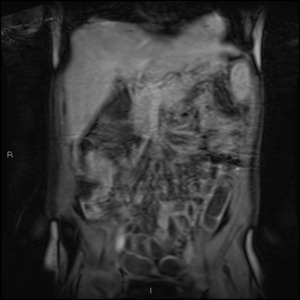
Fig. 6:
Coronal T1 FS VIBE post contrast.
Both normal and abnormal bowel...

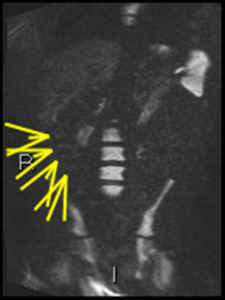
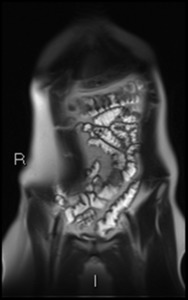
Fig. 5:
Coronal True FISP image showing chemical shift artefact

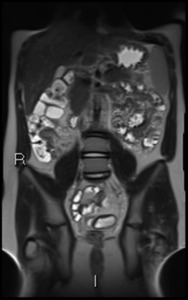
Fig. 7:
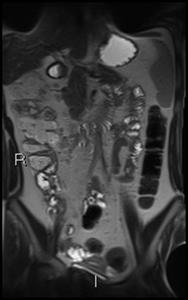
Coronal T2 HASTE image.
Patient presenting with rectal bleeding.
Adequate...

Fig. 8:
b1300 coronal DWI shows colonic haustral high signal. This was initially...

Fig. 9:
Coronal DWI b1300 showing haustral diffusion abnormality.
Endoscopy shows...
 to decide if inflammation is present")
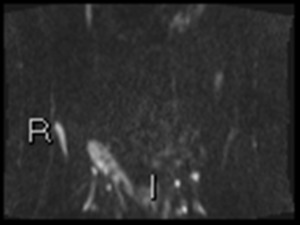
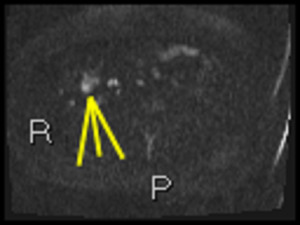
Fig. 3:
b1300 DWI shows high signal in terminal ileum
Absolute ADC measurement of...

Fig. 12:
Coronal HASTE shows thickened terminal ileum

Fig. 13:
Coronal HASTE shows extensive large bowel wall thickening

Fig. 14:
b1300 DWI confirms inflammation in ileum and left colon

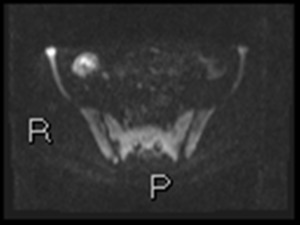
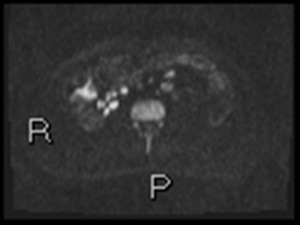
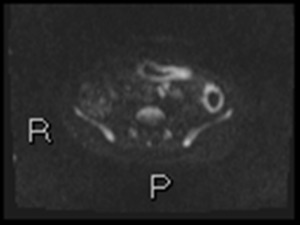
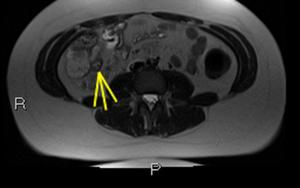
Fig. 15:
Axial DWI b1300 shows ileal inflammation.
Nodal high signal is noted. Unlike...

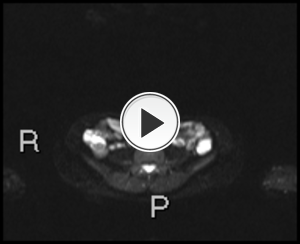
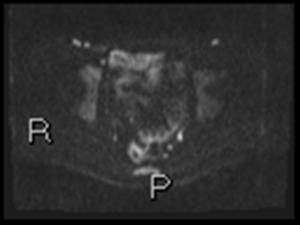
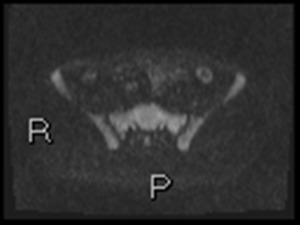
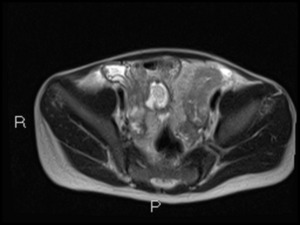
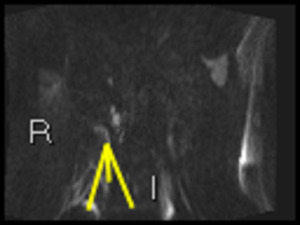
Fig. 16:
Axial b1300 DWI shows circle of hyperintensity in left iliac fossa. This is...

Fig. 17:
Coronal T1 Fat Sat VIBE post contrast images.
Increased enhancement in ileum...

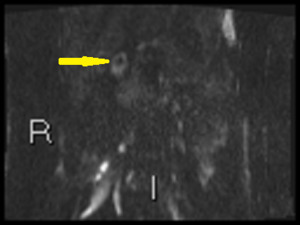
Fig. 18:
Coronal HASTE images show ileal inflammation

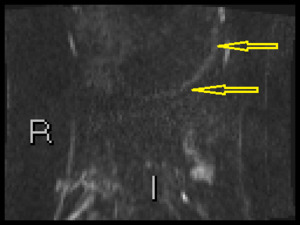
Fig. 19:
Coronal HASTE images show ileal inflammation. Deep ulcer noted

Fig. 20:
Coronal True FISP image shows abnormal configuration of terminal and distal...
")
Fig. 21:
Coronal True FISP image shows abnormal configuration of terminal and distal...

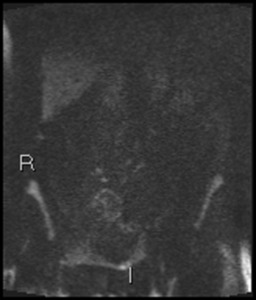
Fig. 22:
Coronal b1300 DWI images show minor diffusion abnormality at site of fistula

Fig. 23:
Thickened left flank bowel loop with surrounding echogenic fat.
Initially this...

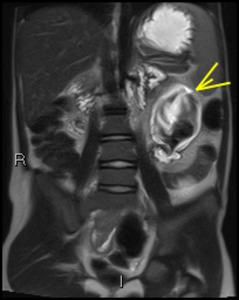
Fig. 25:
Dilated jejunal loop
Low signal seen in the distended bowel loop is caused by...

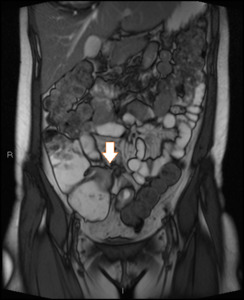
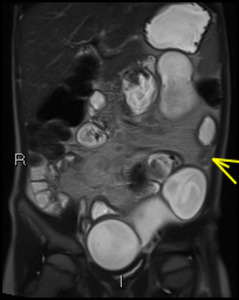
Fig. 26:
Arrowhead denotes a fleshy stricutre with multiple dilated bowel loops giving a...

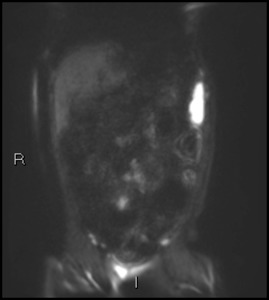
Fig. 27:
Coronal DWI b1300 shows multiple areas of high signal consistent with...

Fig. 28:
Axial HASTE images showing bowel wall thickening and oedema in distal jejunum

Fig. 29:
b1300 axial DWI correlates the wall inflammation

Fig. 32:
b1300 DWI shows gastric inflammation in a 13 year old boy

Fig. 33:
The same 13 year old boy has high signal in proximal duodenum on b1300 coronal...

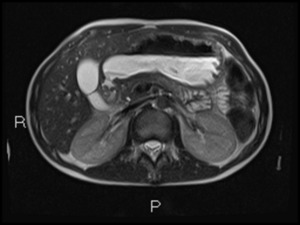
Fig. 34:
Axial T2 HASTE shows duodenal dilatation

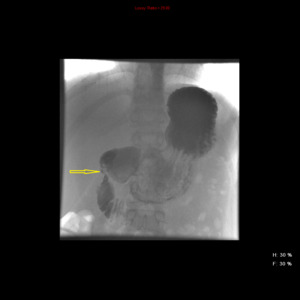
Fig. 35:
Contrast meal confirms D1 stricture

Fig. 41:
Axial T2 HASTE images show terminal ileal wall thickening