ECR 2020 / C-01241
Capsule endoscopy: The use of imaging pre and post procedure to assess risks and manage complications
Congress:
ECR 2020
Poster Number:
C-01241
Type:
Educational Exhibit
Keywords:
Not applicable, Inflammation, Endoscopy, CT-Enterography, CT, Gastrointestinal tract, Abdomen, GI Tract
Authors:
V. Naidu1, S. Zafar1, G. Kakar1, O. Y. Wong2, H. Steinitz2, K. Planche2; 1London/UK, 2Royal Free Hospital NHS Trust /UK
DOI:
10.26044/ecr2020/C-01241

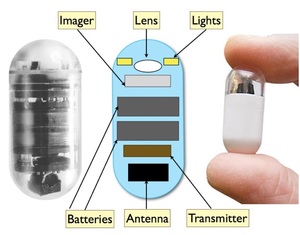
Fig. 1:
Internal components of a video capsule endoscope

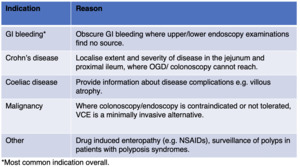
Fig. 2:
Indications for capsule endoscopy
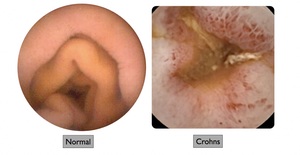
 versus ulceration in a patient with Crohn’s disease (right).")
Fig. 3:
Select images from VCE study demonstrating normal gastrointestinal mucosa...

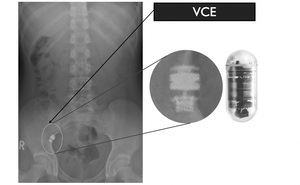
Fig. 4:
A terminal ileal stricture in a 16-year-old Crohn’s disease patient causes...

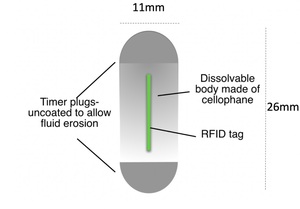
Fig. 5:
Patency capsule with RFID tag

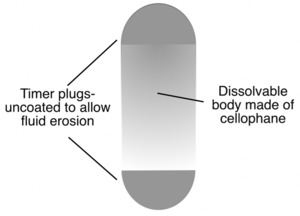
Fig. 6:
Tagless patency capsule

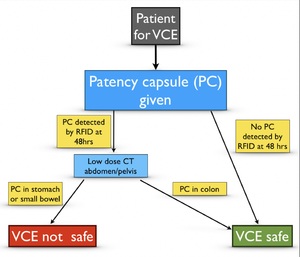
Fig. 7:
Royal Free Hospital protocol for investigations prior to VCE