ECR 2020 / C-01241
Capsule endoscopy: The use of imaging pre and post procedure to assess risks and manage complications
Congress:
ECR 2020
Poster Number:
C-01241
Type:
Educational Exhibit
Keywords:
Not applicable, Inflammation, Endoscopy, CT-Enterography, CT, Gastrointestinal tract, Abdomen, GI Tract
Authors:
V. Naidu1, S. Zafar1, G. Kakar1, O. Y. Wong2, H. Steinitz2, K. Planche2; 1London/UK, 2Royal Free Hospital NHS Trust /UK
DOI:
10.26044/ecr2020/C-01241
, which is abnormally thick walled (C). One of the capsules had later perforated into the bladder.")
Fig. 8:
The importance of pre and post procedural imaging
A 77-year-old patient who...
:
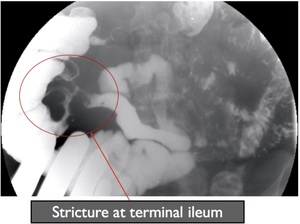
66-year-old Crohn’s disease patient with a terminal ileal stricture. A SBFT cannot determine the functional patency of this stricture and thus a clinical decision for VCE cannot be made - INDETERMINATE FOR VCE")
Fig. 9:
Small bowel follow-through (SBFT):
66-year-old Crohn’s disease patient with...

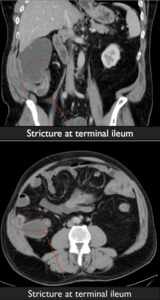
Fig. 10:
CT Enterography- 66-year-old with Crohn’s disease demonstrating mucosal...

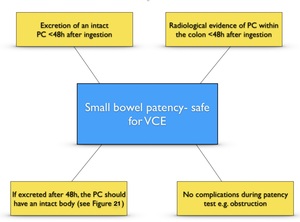
Fig. 12:
Patency test criteria for proving functional small bowel patency

Fig. 13:
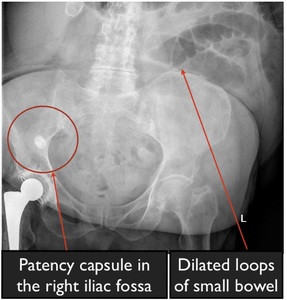
Pitfall of the abdominal radiograph. Abdominal radiograph of a 16-year-old with...

Fig. 14:
Radiographs alone cannot ascertain whether it is safe to proceed with VCE, as...

Fig. 15:
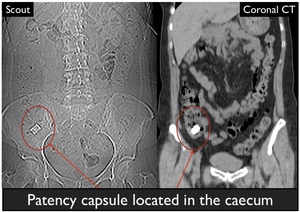
29-year-old with history of previous ileal surgery undergoing a patency capsule...

Fig. 16:
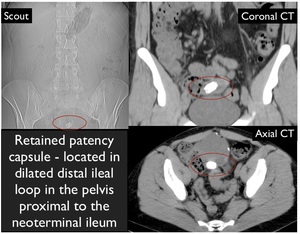
69-year-old patient with a retained patency capsule. Scout image finds the...

Fig. 18:
85-year-old patient undergoing a PC test prior to VCE for suspected...
.
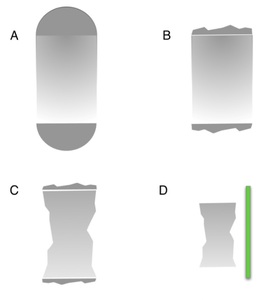
A and B facilitate VCE.
C and D preclude VCE.
A) Intact PC and intact plugs
B) Intact body with eroded plugs
C) Eroded PC body
D) Empty shell and RFID tag
Original found at:
Metronic. The PillCam™ Patency Capsule is the best way to prove GI Patency prior to a CE Exam. In: Medtronic, editor. https://diagmedhealthcare/wp-content/uploads/2017/09/PillCam-Patency-Brochurepdf2016.")
Fig. 21:
Patency capsule after egestion. Modified illustration from Medtronic’s...

Fig. 22:
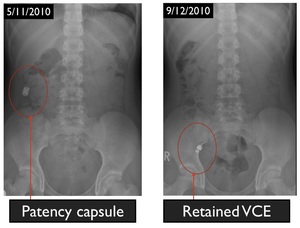
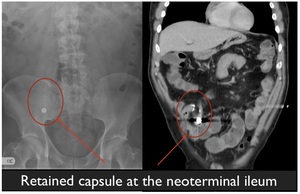
54-year-old patient with Crohn’s disease and previous small bowel surgery....
. An abdominal radiograph (B) found a radiodense structure in the mid-abdomen. This was demonstrated on CT enterography to represent retained video capsule endoscope (C), proximal to a small bowel stricture. The patient had forgotten that this procedure had occurred 3 years earlier.")
Fig. 24:
20-year-old patient with stricturing Crohn’s disease. Routine MR enterography...
 finds the patency capsule to be within the left upper quadrant and thus a limited CT abdomen/pelvis was performed to minimise dose. A high-density ovoid structure is seen in the stomach (B), which was presumed to represent a retained patency capsule. However, the patency capsule is actually visualised in the descending colon, and the high-density structure in the stomach represents a pill (this is not seen on the scout image).")
Fig. 27:
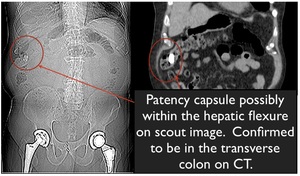
23-year-old patient undergoing a patency capsule test. CT scout image (A) finds...