ECR 2020 / C-04097
Prionic diseases: to the search and capture of diffusion restriction
Congress:
ECR 2020
Poster Number:
C-04097
Type:
Educational Exhibit
Keywords:
Neuro, Neuroradiology brain, MR-Diffusion/Perfusion, Imaging sequences, Infection, Not applicable
Authors:
A. Hilario Barrio1, E. Salvador1, P. Martín Medina2, L. Koren1, J. M. Millan1, A. Martinez de Aragon1, P. M. Latorre Brajovic3, L. Hernandez Martinez1, A. Ramos Gonzalez1; 1Madrid/ES, 228041/ES, 3Santiago de Chile/CL
DOI:
10.26044/ecr2020/C-04097

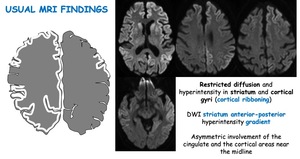
Fig. 3:
Usual MRI Findings. Restricted diffusion and hyperintensity in striatum and...

Fig. 4:
Usual MRI Findings. Perirolandic area usually spared; absence of limbic...

Fig. 5:
Serial MRI reveals that both cortical and basal ganglial DWI hyperintensities...

Fig. 6:
Cerebral atrophy with thickening of the cerebral cortex in advanced stage of...

Fig. 7:
Unusual MRI findings. Pulvinar and double hockey stick signs

Fig. 8:
Unusual MRI findings. Hallmark of cerebellar involvement in sCJD is atrophy

Fig. 9:
Differential diagnosis of sCJD. Severe hypoxic ischemic encephalopathy

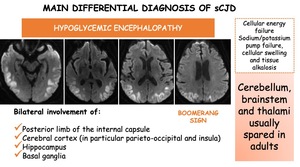
Fig. 10:
Differential diagnosis of sporadic Creutzfeldt-Jakob disease. Hypoglycemic...

Fig. 11:
Differential diagnosis of sCJD. Autoimmune-mediated encephalitis

Fig. 12:
Differential diagnosis of sCJD. Herpes simplex encephalitis

Fig. 13:
Differential diagnosis of sporadic Creutzfeldt-Jakob disease. Postictal state

Fig. 14:
Differential diagnosis of sCJD. SMART syndrome

Fig. 15:
Differential diagnosis of sporadic Creutzfeldt-Jakob disease. Mitochondrial...