As in adults, the most common sites of childhood thrombosis are the deep venous system of the lower limbs and pulmonary arteries and its branches. Thus, abdominal vessels thrombosis (AVT) is a rare entity. On the other hand, one should be able to diagnose it mainly because of its high morbidity.
The abdominal vessels thrombosis may be a consequence of an underlying prothrombotic disorder, or secondary to the use of vascular catheters in hospitalized, which explains why it usually carries a poorer prognosis than the most common types of thrombosis, such as deep vein thrombosis (DVT) and pulmonary thromboembolism (PTE).
90% of patients with AVT have a congenital risk factor for thrombosis, and conditions such as antiphospholipid antibody syndrome or protein C / protein S deficiency or other thrombophilias may be related. In addition, acquired causes such as sepsis, trauma, neoplasms and central venous catheterization play a major role in the pathophysiology of this disease, the latter being also one of the causes of AVT increasing prevalence.
Additional risk factors are younger age, low body mass index and recent surgery.
It is important to highlight the high rate of recurrence in these patients, which reached 21% in a seven years of follow-up.
Central catheterization in the neonatal care is commonly related to the occurrence of thrombosis, and is worth understanding: the catheter travels from the umbilical vein into the left portal vein, then passing through the venous duct and ideally terminating in the superior vena cava / right atrium.
Inferior Vena Cava Thrombosis
Is a condition commonly caused by extension of ilio-femoral deep vein thrombi which are a common complication of femoral vein catheterization.
Venous catheterization may be the main risk factor for neonatal thrombosis due to the underdeveloped newborn coagulation system in addition to the intima damage and the concomitant use of hyperosmolar pH solutions may result in clotting cascade activation and thrombosis. Congenital inferior vena cava atresia may present with calcified IVC thrombosis in neonates, but it is a rare condition.
It may cause the Inferior vena cava syndrome (IVCS), evolving for acute and rapid development of tachycardia, peripheral edema, and renal failure.
Ultrasonographic findings include thrombus appearing as a hyperechogenic image filling and tapering the venous lumen.

Fig. 1: Common Iliac Veins and Inferior Vena Cava Thrombosis
References: São Paulo
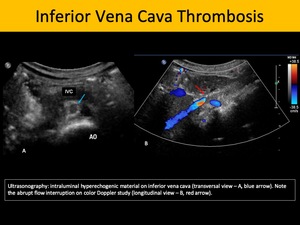
Fig. 2: Inferior Vena Cava Thrombosis
References: São Paulo
Renal Vein Thrombosis
It is the most prevalent site of AVT site among children. Risk factors include all the aforementioned conditions, as well as dehydration, maternal diabetes, and preeclampsia. The clinical presentation is depicted by the triad: abdominal mass, thrombocytopenia and hematuria. If this condition is not treated, it may progress to hypertension and renal failure. The left renal vein is the most commonly affected.
Sonography is highly specific for this diagnosis in children as it can evidence increased renal dimensions, loss of corticomedullary differentiation, intraluminal thrombus, disturbance of the venous spectral waveform pattern, occasionally presenting reversed diastolic flow
Less frequently, one may find curvilinear hyperechogenic formations which represent the thrombosed arcuate vessels.
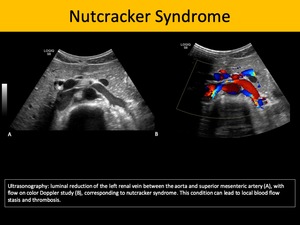
Fig. 3: Nutcracker Syndrome
References: São Paulo
Portal Vein Thrombosis
It is the second most common type of AVT in children and approximately 75% of cases are related to umbilical venous catheterization. When unrelated to catheters, it may be an incidental finding on abdominal sonography of infants with congenital anomalies, thrombocytopenia, cardiopathy, perinatal asphyxia, infections, prematurity. It may cause elevated liver enzymes and hyperbilirubinemia.
The catheter related thrombosis often occurs in the left portal vein. Therefore, the most frequent complication is left hepatic lobe atrophy as well as portal hypertension.
Sonography is the primary screening method for this entity, as it may depict hyperechogenic intraluminal formation compatible with thrombus, and lack of color Doppler flow. Chronic portal vein thrombosis may also exhibit cavernous transformation of the portal vein and stigmata of portal hypertension. Abdominal CECT or magnetic resonance image (MRI) are useful to complement the evaluation of the parenchyma for cirrhosis or concomitant masses.
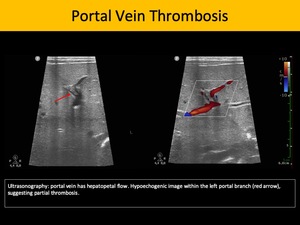
Fig. 5: Portal Vein Thrombosis
References: São Paulo
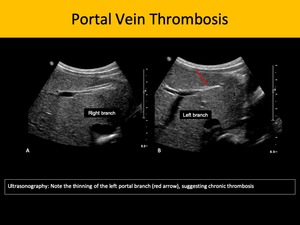
Fig. 6: Portal Vein Thrombosis
References: São Paulo
Splenic Vein Thrombosis
It is usually secondary to pancreatitis, malignancies and direct extension portomesenteric venous thrombosis. Pancreatitis in children main causes are trauma, cholecystolithiasis and medications. The sonography is readily available and detects intraluminal thrombus. Contrast-enhanced computed tomography (CECT) has greater sensitivity for splenic vein thrombosis, particularly in the acute phase, as it may easily depict associated findings, such as pancreatitis, pseudocysts, peripancreatic collection or necrosis.
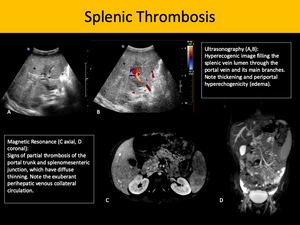
Fig. 7: Splenic Thrombosis
References: São Paulo
Superior mesenteric vein thrombosis
It may either be an extension of a portal vein thrombosis or be the primary site itself. Clinically, it presents as abdominal distension, stigmata of small bowel ischemia and severe abdominal pain. In this pathology, CECT and MRI are significantly sensitive for diagnosis and useful for follow-up, since those methods can detect pneumatosis, pneumoperitoneum and segmental or diffuse small bowel wall thickening and increased parietal enhancement.
Sonography has low sensitivity and specificity for this diagnosis. Abdominal bloating associated with small bowel wall thickening the usual sonographic findings.
Budd-Chiari Syndrome
It refers to the clinical syndrome caused by hepatic veins or inferior vena cava thrombosis. Predisposing factors are polycythemia rubra vera, paroxysmal nocturnal hemoglobinuria, dehydration, sepsis and other thrombophilic conditions. In the acute phase, it causes hepatocyte necrosis and, chronically, one may present portal hypertension with subsequent liver cirrhosis. Massive splenomegaly is an important feature on physical examination.
Sonography shows thrombosis in the hepatic veins or inferior vena cava, lacking the usual triphasic waveform pattern of the former and low or absent flow in the latter, as well as morphological changes of the hepatic parenchyma under B-mode evaluation and abundant collateral vessels. Hepatofugal flow in the portal vein is a frequent finding as the disease progresses to portal hypertension.
Aortic Thrombosis
The most common cause of aortic thrombosis in neonatal patients is umbilical artery catheterization, which is commonly used to obtain arterial blood sampling or as an access to fluid therapy. Catheterization-related aortic thrombosis occurs typically in neonates, as this type of procedure is rarely performed in children older than 10 days of age. As such, sonography is the safest and fastest method for aortic evaluation, and the thrombus may appear as either hypo, iso or hyperechogenic intraluminal formations.
Differential diagnoses include aortic coarctation, aortic pseudo-dissection.
Other risk factors such as polycythemia rubra vera, cardiopathy, patent ductus arteriosus, thrombophilias and sepsis are also implicated in aortic thrombosis, and should be suspected in older or non-catheterized patients presenting this entity.
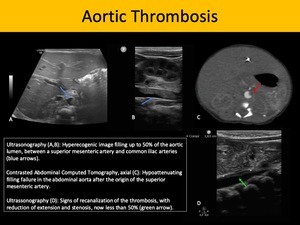
Fig. 8: Aortic Thrombosis
References: São Paulo








