ECR 2020 / C-04423
Imaging features of Alagille Syndrome: focus on a rare but important condition.
Congress:
ECR 2020
Poster Number:
C-04423
Type:
Educational Exhibit
Keywords:
Transplantation, Genetic defects, Diagnostic procedure, Ultrasound, MR, CT, Paediatric, Liver, Abdomen, Not applicable
Authors:
M. Milazzo1, A. Di Piazza1, C. Cannataci2, V. Carollo3, S. Caruso4, G. Marrone1, G. Gentile1, R. Miraglia5; 1Palermo/IT, 2Msida/MT, 3Palermo (PA)/IT, 4Palermo (PA), italy/IT, 5Palermo /IT
DOI:
10.26044/ecr2020/C-04423
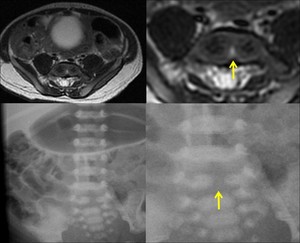
 is a type of vertebral anomaly that results from the failure of fusion of the lateral halves of the vertebral body because of persistent notochordal tissue between them.")
Fig. 3:
Butterfly vertebra (seen on MRI T2 weighted imaging and x-ray) is a type of...
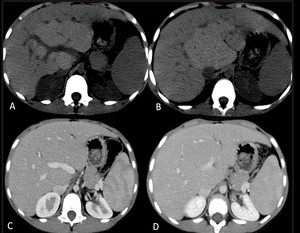
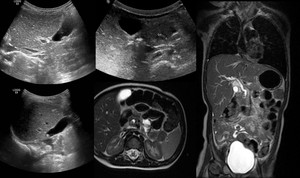
 and after (C-D) administration of intravenous contrast showing a large hepatic nodule surrounding the right portal vein, a typical site for nodules in Alagille syndrome. The portal vessels go through the mass and are not altered by it, a finding which points to benignity and should suggest the diagnosis of a large regenerative nodule as opposed to a malignant lesion.")
Fig. 4:
5 month old infant with end-stage liver disease: Pre-transplant assessment MDCT...
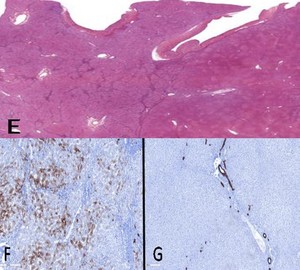
 shows two different areas: duttopenic hepatic parenchyma and on the right the pseudo-nodular area, corresponding to the nodule seen at CT, whict at microscopic vision shows an overall preserved architecture with normal representation of biliary ducts in the portal sections. (F) CK7 underlines the loss of the bile ducts in the areas of affected hepatic parenchyma, ductal reaction and hepatocyte biliary metaplasia (G) in contrast in the spared parenchyma, CK7 colors the normal bile ducts.")
Fig. 5:
Same case on the explant: Hematoxylin- Eosin panoramic photo (E) shows two...

Fig. 6:
Volume Rendering: Stenoses at lobar and segmental pulmonary arteries in 8...
 is a congenital biliary disorder, which is characterized by an absence or severe deficiency of the extrahepatic biliary tree. It is one of the most common causes of neonatal cholestasis, often causing cirrhosis immediately and leading to death and accounts for over half of children who undergo liver transplantation. US criteria: Echogenic fibrous tissue anterior to the portal vein: triangular cord sign: larger hepatic arterial caliber; gallbladder ghod triad (atretic gallbladder, length less than 19 mm; irregular or lobular contour; lack of smooth/complete echogenic mucosal lining with an indistinct wall).")
Fig. 7:
Biliary atresia (BA) is a congenital biliary disorder, which is characterized...

Fig. 8:
MRI; M, 7 month: gallbladder sketch in cystic fibrosis.

Fig. 9:
US nad MRI: M, 3yr-old choledochal lithiasis.
 according to Todani (1977):
I: 80-90% of the injuries ; a- saccular dilations that involve the entire extrahepatic biliary tract or most of it; b- saccular dilations involving a limited portion of the biliary tract; c- fusiform dilations involving most of the extrahepatic biliary tract.
II: Isolated diverticulum protruding from the wall of the common bile duct; they can be sessile or connected to the common bile duct by a narrow peduncle.
III: Choledococele, usually found in the intraduodenal portion of the common hepatic duct.
IVa: Multiple dilations of the intra and extrahepatic bile ducts. IVb: Multiple dilations involving only the extrahepatic biliary tract.
V: Caroli disease.")
Fig. 10:
Classification of choledochal cysts (5 types) according to Todani (1977):
I:...
, also called anomaly of the bilio-pancreatic junction.
The presence of an anomaly of the bilio-pancreatic junction determines the reflux in the choledochus of the enzymes secreted by the pancreas, causing the formation of a cyst. Chronic inflammation of the bile walls is considered a risk factor for neoplastic degeneration.")
Fig. 11:
Choledochal cyst: congenital dilation fusiform or focal of the extrahepatic...