ECR 2020 / C-06111
Chemo-induced hepatotoxicity: a survival guide.
Congress:
ECR 2020
Poster Number:
C-06111
Type:
Educational Exhibit
Keywords:
Oncologic Imaging, Abdomen, Liver, Oncology, CT, MR, Ultrasound, Complications, Diagnostic procedure, Biological effects, Drugs / Reactions, Neoplasia, Not applicable
Authors:
M. LETURIA ETXEBERRIA, F. J. Barba Tamargo, A. Serdio, M. Gredilla, J. Burgos Ruiz, J. Badiola Molinuevo, A. Luis Fernández, A. Aguado, A. agote; Donostia - San Sebastián/ES
DOI:
10.26044/ecr2020/C-06111

Fig. 3:
Classic and New Chemotherapeutic agents

Fig. 4:
Chemo-induced hepatotoxicity

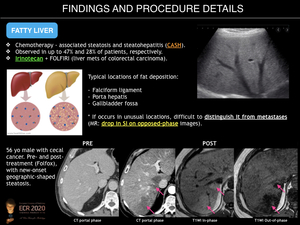
Fig. 5:
Fatty Liver

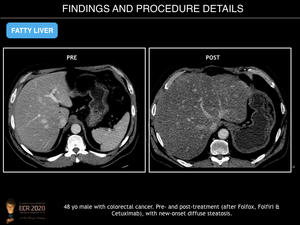
Fig. 6:
Fatty Liver
")
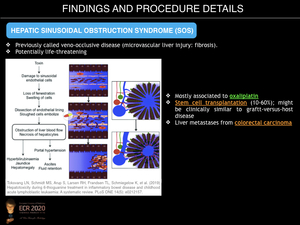
Fig. 7:
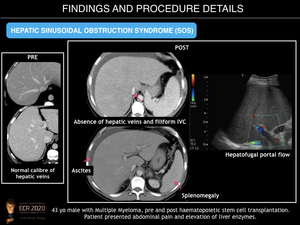
Hepatic Sinusoidal Obstruction Syndrome (SOS)
")
Fig. 8:
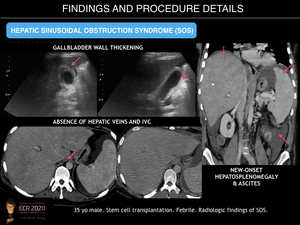
Hepatic Sinusoidal Obstruction Syndrome (SOS)
")
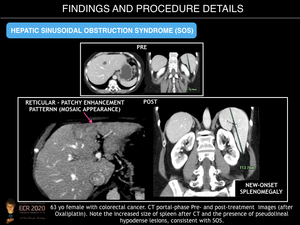
Fig. 9:
Hepatic Sinusoidal Obstruction Syndrome (SOS)
")
Fig. 10:
Hepatic Sinusoidal Obstruction Syndrome (SOS)

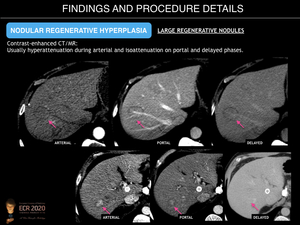
Fig. 11:
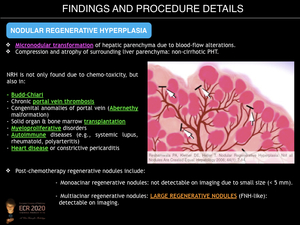
Nodular Regenerative Hyperplasia

Fig. 12:
Nodular Regenerative Hyperplasia

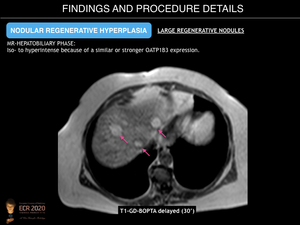
Fig. 13:
Nodular Regenerative Hyperplasia

Fig. 14:
Nodular Regenerative Hyperplasia

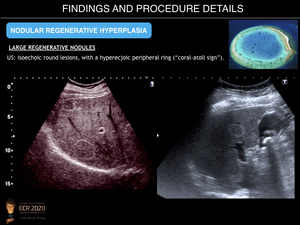
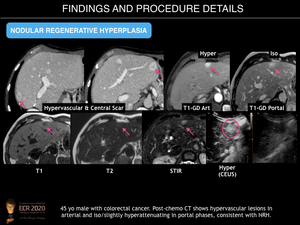
Fig. 15:
Nodular Regenerative Hyperplasia

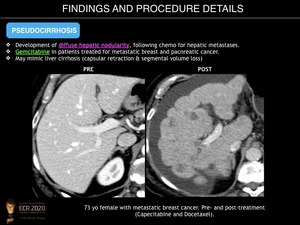
Fig. 16:
Pseudocirrhosis

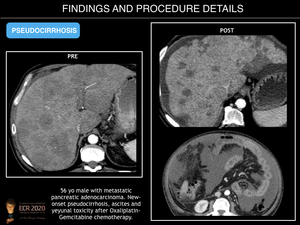
Fig. 17:
Pseudocirrhosis

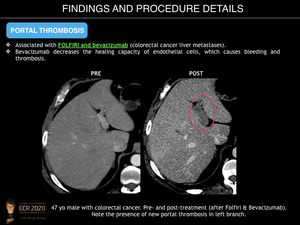
Fig. 18:
Portal Thrombosis

Fig. 19:
Chemo-induced hepatotoxicity: summary table

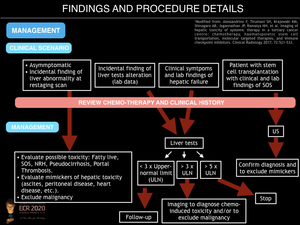
Fig. 20:
Management of chemo-induced hepatotoxicity.