ECR 2020 / C-06578
Pattern Recognition of Non-Mass Enhancements on Breast MRI – A Pictorial Review with Radiologic-Pathologic Correlation.
Congress:
ECR 2020
Poster Number:
C-06578
Type:
Educational Exhibit
Keywords:
Not applicable, Cancer, Education, MR, Mammography, Breast
Authors:
K. S. Loi1, W. Y. Chan2, M. T. Ramli Hamid3, K. Rahmat2; 1Federal Territory of Kuala Lumpur/MY, 2Kuala Lumpur/MY, 3Sungai Buloh/MY
DOI:
10.26044/ecr2020/C-06578

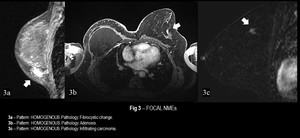
Fig. 3:
Focal NMEs

Fig. 4:
Linear NMEs

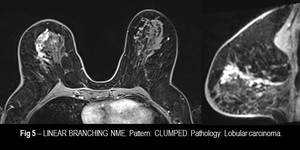
Fig. 5:
Linear Branching NME

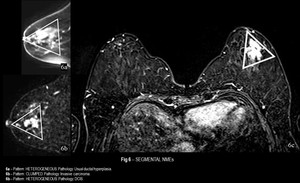
Fig. 6:
Segmental NMEs

Fig. 7:
Regional NMEs

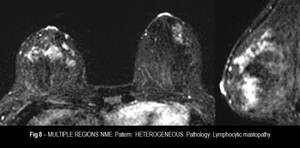
Fig. 8:
Multiple Regions NME

Fig. 9:
NMEs with homogenous enhancement pattern

Fig. 10:
NMEs with heterogeneous enhancement pattern

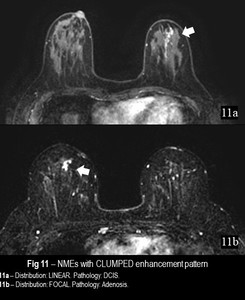
Fig. 11:
NMEs with clumped enhancement pattern

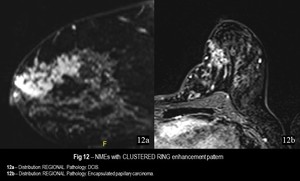
Fig. 12:
NMEs with clustered ring enhancement pattern

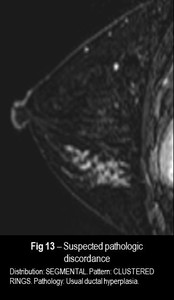
Fig. 13:
Suspected pathologic discordance