ECR 2020 / C-07465
Doppler ultrasound in the evaluation of the revascularized carotid postendarterectomy. What should you know?
Congress:
ECR 2020
Poster Number:
C-07465
Type:
Educational Exhibit
Keywords:
Not applicable, Arteriosclerosis, Surgery, Complications, Ultrasound-Spectral Doppler, Ultrasound-Colour Doppler, Ultrasound, Vascular
Authors:
H. Varela1, J. Crosta1, P. TARRAGA TOLABA1, A. M. perdomo olivera1, J. A. Palacios Cuesta2, N. H. C. P. CUSSA NAIZIR2, D. Vargas Flores1, Y. P. Narváez Rojas1, L. Borrino1; 1Buenos Aires/AR, 2Pablo Nogues/AR
DOI:
10.26044/ecr2020/C-07465
 B: suture stitches (pink arrows) D: Adequate flow with color doppler. No stenosis")
Fig. 4:
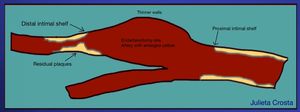
Normal findings. Endarterectomy of 3 years of evolution. A- C distal shelf of...

Fig. 5:
Normal findings. The artery caliber is enlarged. The pink arrows are showing...

Fig. 6:
Normal findings. A: ICA after endarterectomy of 5 years of evolution. B:...
The arrow points out several calcified atheromatous plaques as a sign of recurrence of basal atherosclerosis.")
Fig. 7:
Normal findings. A: Enlarged artery at the ECA site. Thinner walls. B: normal...
 after endarterectomy. The distal shelf lesion is seen (pink arrows), where is the upper limit of the removal of the intimal layer. This is the point where a careful evaluation is needed, because residual plaque or restenosis happens here.")
Fig. 8:
Right Internal Carotid artery (RICA) after endarterectomy. The distal shelf...
 of a venous patch of an endarterectomy RICA: right internal carotid artery. RCCA: right common carotid artery.")
Fig. 9:
Suture stitche (pink arrows) of a venous patch of an endarterectomy RICA: right...
")
Fig. 10:
Patient with right endarterectomy. Synthetic patch of PTFE seen at the wall of...
 at the posterior wall of the right Common Carotid artery (RCCA) after two months of endarterectomy. Color Doppler shows flow within the lesion. It seems to be an ulcer caused by the rupture of the intima at the point where the clamp is set during the surgery. It remained stable after several months. There were no further complications.")
Fig. 11:
Clamp lesion.Two intimal flaps are seen as an ulcer (pink arrows) at the...
. No liquid is seen adjacent to the vessel. This findings could be a sign of infection. It needs follow up.")
Fig. 12:
Irregular patch (pink arrows). No liquid is seen adjacent to the vessel. This...
 with the artery.")
Fig. 13:
Pseudoaneurism. A: Yin-yang sign showing flow turbulence at the false cavity....

Fig. 14:
Thrombosis of the artery lumen 1 month postendarterectomy. A: pink arrow shows...
. C: High velocities in the spectral Doppler. PSV 304 cm/s EDV 106 cm/s.
This is a > 70% stenosis, according to the velocities.")
Fig. 15:
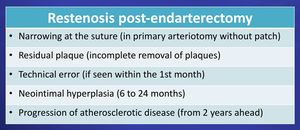
Restenosis at the ECA site. A-B: Thrombosis of the lumen with narrowing of the...
.")
Fig. 16:
1 year of surgery. Hyperplasia neointimal seen at the posterior wall of the...
")
Fig. 17:
Hyperplasia neointimal seen at the walls of the artery postECA (pink arrows)
 is observed, as well as signs of > 70% obstruction in right internal carotid artery (RCIA) (B). Narrowing of the lumen is observed with color Doppler (B) (pink arrow). C: Right common carotid artery (RCCA): PSV: 42 cm/s. D: the velocities are increased at the area of higher narrowing (PSV 339 cm/s EDV: 126 cm/s) as well as the S/S ratio of 8.")
Fig. 19:
Right carotid bifurcation after 16 months after endarterectomy. A: Neointimal...

Fig. 20:
Complicated ECA. A and B: 12 months after surgery. A color flow gorge is seen...