Magnetic field strength:
One of the most frequently discussed topics of prostate mpMRI is whether to use 1.5T or 3T MRI field strength. A comparison between the 1.5T and 3T MRI by Ullrich et al. [8] showed:
-
T2-weighted images (T2WI):
Comparable “signal-to-noise” (SNR) and “contrast-to-noise” (CNR)
-
Diffusion-weighted images (DWI):
SNR and CNR significantly lower at 1.5T
An example of 1.5T versus 3T MRI of the prostate in the same patient is shown in Fig. 1.
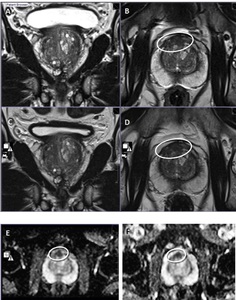
Fig. 1: Magnetic field strength 3T MRI vs 1.5T MRI.
1A and 1B. 3T-axial and coronal T2WI, and 1C and 1D. 1.5T-axial and coronal T2WI. Anterior transition zone (TZ) lesion (circle). 1E. 3T-axial ADC-map. 1F. 1.5T-axial ADC-map. Biopsy showed an anterior Grade Group 1 (Gleason score 3+3) anterior TZ cancer.
References: Paul Strickland Scanner Centre, Mount Vernon Hospital - Northwood/UK
Gradient strength:
The SNR and CNR are dependent on the maximum value- and rise-time of the magnetic field gradients. Especially for DWI, where image quality highly depends on the gradient strength [9-12]. Stronger gradients allow shorter echo time (TE), enabling a higher SNR and better DWI quality [13, 14].
Receiver coils:
The most commonly used receiver coil is a body phased array coil in combination with a spine coil. Many centers also employ an endorectal coil (ERC). The PI-RADS Committee does not prescribe the use of ERC, stating that reliable, satisfactory results can be obtained with both 1.5T and 3T without the use of an ERC [6]. This position is supported by a systematic review performed by Fusco et al. [15]. Fig. 2 displays an example of a patient who underwent mpMRI of the prostate with and without the use of an ERC.
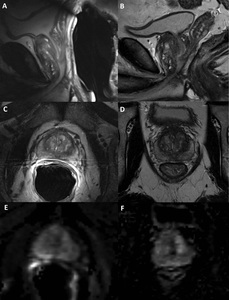
Fig. 2: ERC vs non-ERC MRI of the prostate.
This image shows a patient who underwent a 3T MRI with ERC (A,C,E) and without ERC (B,D,F).
T2WI sagittal (A,B), T2WI axial (C,D) and calculated b1400 (E,F) images are shown. The images with the use of an ERC contain image artifacts and the prostate is noticeably compressed whereas the images without the use of an ERC are free from artifacts.
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
Patient preparation:
The different patient preparation methods for mpMRI of the prostate are discussed below. A summary of recommendations can be found in Table 1.

Table 1: Summary of evidence and guidelines for the acquisition of mpMRI of the prostate.
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
Antispasmodic agents:
Administration of an antispasmodic agent can prevent blurring of images by decreasing bowel motility. The effect of antispasmodic agents on mpMRI[16]:
Fasting:
Fasting was not mentioned in PI-RADS v2. Evidence for the use of fasting to decrease rectal air or bowel movement is lacking.
Preparation enema:
Rectal distension has a significant negative effect on the quality of both T2WI and DWI [17]. To optimize image quality, bowel preparation prior to prostate mpMRI should be considered. Lim et al. [18] showed that preparatory cleansing enemas did not improve image quality or reduced artifacts in 3T prostate mpMRI. However, van Griethuysen et al [19] investigated the use of a preparatory microenema shortly before the DWI sequence. The microenema consisted of a 5ml solution that was self-administered by the patient + 15 min prior to acquisition. This significantly reduced both the incidence and the severity of gas-induced artifacts.
Rectum catheter:
Air within the rectum can cause susceptibility artifacts that distort DWI. Caglic et al. [17] reported a strong positive correlation between increased rectal feces and air and DWI distortion. To reduce these artifacts, the amount of air in the rectum can be removed by inserting a rectal catheter. Fig. 3 shows the effect of using a rectal catheter.
Refraining from ejaculation:
Several articles have examined the influence of ejaculation prior to MRI of the prostate. The main findings were a significant reduction in seminal vesicle (SV) volume after ejaculation and, therefore, decreased diagnostic evaluation of potential SV invasion in patients with known cancers [20-22].
Acquisition protocol:
According to the PI-RADS v2.1 recommendations, the minimal protocol consists of a combination of high-resolution T2WI in at least two planes, and two functional MRI techniques: DWI and dynamic contrast enhanced (DCE) MRI [7]. An overview of setting recommendations is presented in Table 1, and Table 2 presents an overview of the recommended minimal sequence parameters for 3T and 1.5T MRI.

Table 2: Minimal requirements for 3T and 1.5T mpMRI of the prostate
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
T2-weighted imaging:
T2WI shows the prostate’s anatomy and is used for the detection, localization, and staging of PCa.
PCa in the peripheral zone (PZ):
PCa in the transition zone (TZ):
T2WI should always be obtained in the axial plane and at least one orthogonal plane (sagittal or coronal).
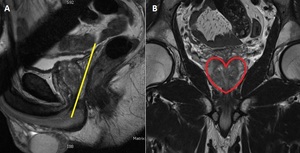
Angulation:
A small shimbox is applied around the prostate to create a homogenous magnetic field to minimize influence of air or bowel movement (Fig. 5).
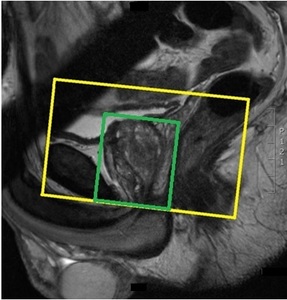
Fig. 5: Angulation of the axial plane (yellow box) and the application of a small shim box around the prostate (green box).
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
A phase encoding direction from left to right is used in the coronal and axial planes to prevent overprojection of motion artifacts from the bowel into the prostate.
Diffusion-weighted imaging:
DWI is an essential sequence for detection and is a predictor of tumor aggression. It reflects the random motion of water molecules and is a key component of the prostate mpMRI examination [6].
PCa demonstrates:
DWI is acquired:
-
In the axial plane
-
With a small shim box in the same position and phase encoding direction as the T2WI [5]
-
Multiple b values, typically b50–100, b400-500, b800, and a high b value of at least b1400 s/mm2
Increasing b values naturally decreases the SNR, to compensate for signal losses it is important to increase the NEX. DWI is very sensitive for artifacts that are caused by field inhomogeneities. Such artifacts can be minimized by using short TE [14]. An example of good versus bad high b-value DWI image quality can be seen in Fig. 6.
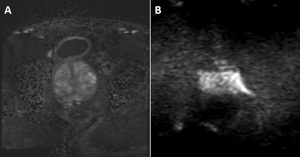
Fig. 6: DWI image quality.
A.DWI b1400 axial image of the prostate with an acceptable image quality. B. DWI b1400 axial image of the prostate with no acceptable image quality because of a lot of noise and a susceptibility artifact.
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
Dynamic contrast enhanced MRI:
DCE-MRI during the administration of a contrast agent shows tissue vascularity and microvessel permeability [5]. DCE is a series of sequential T1-weighted images and is acquired:
Artifact prevention:
The most common artifacts in mpMRI of the prostate are motion and susceptibility artifacts.
Motion causes blurring or ghosting artifacts, and is caused by bowel peristalsis, gland motion, bladder distension, or patient movement. An example of a motion artifact is shown in Fig. 7.
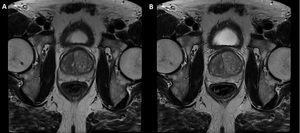
Fig. 7: Motion artifact.
A.T2W axial image of the prostate with a motion artifact. B. T2W image of the prostate in the same patient without motion artifacts.
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
Approaches to minimize motion artifacts:
-
Make the patient as comfortable as possible
-
Administer an antispasmodic agent
-
Decrease acquisition time
Susceptibility artifacts cause distortion of the prostate, especially in DWI. Distortion is caused by local magnetic field inhomogeneities due to rectal air or metal implants [14]. Fig. 8 shows an example of distortion caused by rectal air. An example of hip prosthesis is shown in Fig. 9.
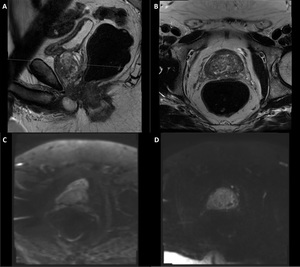
Fig. 8: Distortion caused by rectal air.
A large amount of air in the rectum is visible on the T2 sagittal (A) and T2 axial (B) images. The DWI (C) shows distortion of the prostate caused by rectal air. To decrease the distortion a readout-segmented, multi-shot (RESOLVE) DWI (D) is scanned in the same patient.
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
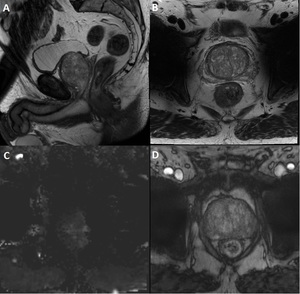
Fig. 9: Influence of hip-prosthesis on image quality.
The T2WI sagittal (A), T2WI axial (B) and the DCE (D) show good image quality to evaluate the prostate. The hip prostheses are displayed as black holes, however they don’t influence the quality of the image in the prostate itself. The DWI (C) is greatly degraded by artifacts and cannot be used for diagnosis.
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL
Approaches to minimize susceptibility artifacts:
MRI radiographers’ training:
Besides proper patient preparation and technical issues, knowledge and dedication of the performing MRI radiographer play a major role in obtaining optimal mpMRI of the prostate. Knowledge of anatomy, pathology, and recognizing specific artifacts and technical knowledge will improve the image quality.

 lesion (circle). 1E. 3T-axial ADC-map. 1F. 1.5T-axial ADC-map. Biopsy showed an anterior Grade Group 1 (Gleason score 3+3) anterior TZ cancer. References: Paul Strickland Scanner Centre, Mount Vernon Hospital - Northwood/UK")
 and without ERC (B,D,F).
T2WI sagittal (A,B), T2WI axial (C,D) and calculated b1400 (E,F) images are shown. The images with the use of an ERC contain image artifacts and the prostate is noticeably compressed whereas the images without the use of an ERC are free from artifacts.
References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL")
 and with (B) the use of a rectum catheter. This demonstrates that, especially in the DWI (right column), susceptibility artifact is present distorting the images where the rectum catheter was not used (arrows), which is considerably improved when the rectum catheter was used. References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL")
. B. Heart shaped coronal view of the prostate with the correct angulation. References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL")
 and the application of a small shim box around the prostate (green box). References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL")
, RadboudUMC - Nijmegen/NL")
, RadboudUMC - Nijmegen/NL")
 and T2 axial (B) images. The DWI (C) shows distortion of the prostate caused by rectal air. To decrease the distortion a readout-segmented, multi-shot (RESOLVE) DWI (D) is scanned in the same patient. References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL")
, T2WI axial (B) and the DCE (D) show good image quality to evaluate the prostate. The hip prostheses are displayed as black holes, however they don’t influence the quality of the image in the prostate itself. The DWI (C) is greatly degraded by artifacts and cannot be used for diagnosis. References: Dept of Radiology and Nuclear Medicine (route 766), RadboudUMC - Nijmegen/NL")
, RadboudUMC - Nijmegen/NL")
, RadboudUMC - Nijmegen/NL")