DONOR EVALUATION
To establish adequacy of donor kidney along with factors that change the operative approach or determine further course of treatment.
USG determines kidney size, presence of lesion that may change course of treatment. 
Fig. 1: CECT in a potential donor shows bilateral polycystic kidney, precluding donation.
References: Chu, Linda C., et al. "Role of MDCT angiography in selection and presurgical planning of potential renal donors." American Journal of Roentgenology 199.5 (2012): 1035-1041
Doppler/MR-Angiography evaluate renal arterial and venous anatomy (accessory arteries/early bifurcations/stenoses/ circum-aortic or retro-aortic renal veins/ number of renal arteries with pre-hilar branching etc and vessel wall condition.
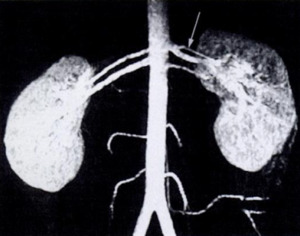
Fig. 2: MIP of Gd enhanced MR angiogram in a donor shows two renal arteries on both sides with early bifurcation of superior renal artery on the left.
References: Low, Russell N., et al. "Potential renal transplant donors: evaluation with gadolinium-enhanced MR angiography and MR urography." Radiology 207.1 (1998): 165-172.
CT angiography is more precise in determining length of the main renal artery before the first parenchymal branch and excluding renal artery or aortic abnormalities.

Fig. 3: Volume rendered CT in a potential renal donor shows beaded appearance of bilateral renal arteries- fibromuscular dysplasia. Patient did not proceed to donation.
References: Chu, Linda C., et al. "Role of MDCT angiography in selection and presurgical planning of potential renal donors." American Journal of Roentgenology 199.5 (2012): 1035-1041
MR urograms detail renal collecting system and MR nephrogram, the renal parenchyma in suspicious cases.
Absolute contraindications-PCKD,solitary/horseshoe and pelvic kidneys. Renal mass,partial duplication,stone,scarring,malrotation and ureteropelvic junction obstruction are relative contraindications.
RECIPIENT EVALUATION
To establish whether transplantation is possible,if presurgical procedures are needed and arrive at best surgical technique suited to the patient1

Fig. 4: Potential kidney recipient with nephromegaly and polycystic kidneys. Coronal reformatted CT shows insufficient space for the renal graft. Right renal nephrectomy was performed to creaste space before transplantation.
References: Catalá, Violeta, et al. "Use of multidetector CT in presurgical evaluation of potential kidney transplant recipients." Radiographics 30.2 (2010): 517-531
Transplanted renal artery is usually anastomosed with external iliac artery/internal iliac artery,rarely with the supra-bifurcational aorta.The renal venous anastomosis is made to the inferior vena cava.
It is therefore vital to check the vascular status of the recipient. Distal aorta, the common iliac vessels, the iliac bifurcation, and the external iliac vessels are evaluated.Calcifications tend to develop in patients on prolonged dialysis and are incompatible sites for anastomosis.
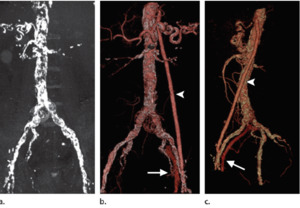
Fig. 5: (a) NECT MIP image in a potntial recipient shows intensive arterial wall calcifications (iliac or splenic anastomosis was not possible). (b, c) Frontal (b) and lateral (c) volume-rendered images show a vascular aortofemoral prosthesis (arrowhead), implanted 2 months before kidney transplantation; correct permeability can be seen. There is early ipsilateral venous enhancement (arrow), which is a normal finding in patients with a vascular aortofemoral prosthesis. Left transplant anatomosis was made with the prosthesis.
References: Catalá, Violeta, et al. "Use of multidetector CT in presurgical evaluation of potential kidney transplant recipients." Radiographics 30.2 (2010): 517-531
Calcification in the internal iliac artery is predictive of plaque in the external iliac artery since internal iliac artery is involved before the external iliac artery1.Any suspicious stenoses/aneurysms/AVF are evaluated further.
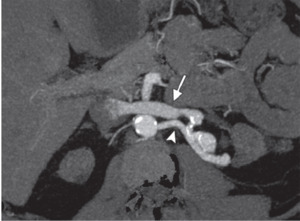
Fig. 6: Arterial phase MIP shows an AVF in a potential recipient with ESRD. Arrowhead=left renal artery,arrow=leftrenal vein with early enhancement. AVF was embolized before transplantation.
References: Catalá, Violeta, et al. "Use of multidetector CT in presurgical evaluation of potential kidney transplant recipients." Radiographics 30.2 (2010): 517-531.
Atherosclerosis, calibre, venous disease iliac fossa patency, prior transplant presence etc.are evaluated in detail on CT-Angiography.
Non-contrast MRA is better for stenosis.
POST-TRANSPLANT EVALUATION
Normal early post-op findings include mildly dilated calyces and pelvis due to oedema at the vesico-ureteric anastomosis.
Doppler USG-Plays a major role in repeated,long term follow up post-transplant. Heterotrophic transplant kidney provides better visualization due to its superficial location in the iliac fossa.
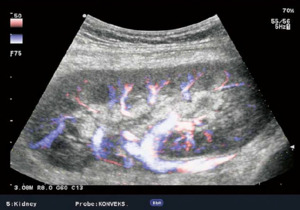
Fig. 7: Colour flow imaging of normal intrarenal vascularization in a transplanted kidney.
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694

Fig. 8: (A)Normal Colour and spectral doppler of the anastomosis of transplant artery on iliac artery (PSV 1.5m/s)
(B) Normal colour and spectral doppler in the renal vein.
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694.
Transplant renal arteries should be visualised throughout their course, albeit sometimes difficult due to tortuous course. PSV>2 m/s and ratio of PSV(renal artery) to PSV(iliac artery) >2.5:1 suggests renal artery stenosis2. Resistive indices of the segmental,interlobar and arcuate arteries should be< 0.70 and RI >0.90 is 100% predictive of acute rejection2.
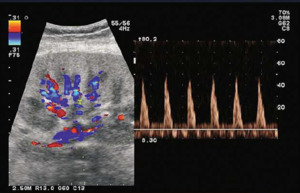
Fig. 9: Spectral doppler of the intrarenal arteries without diastolic flow, even with triphasic spectrum indicate acute rejection.
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694
Iliac artery is mapped to rule out stenosis or occlusion by demonstrating normal triphasic waveform and flow velocity.Renal vein/ Iliac vein thrombosis should be excluded by colour flow mapping.
CT/MRI is performed in unsatisfactory USG (obese).
Complications post-transplant can be divided into-
Parenchymal Abnormalities
1. Hyperacute rejection- Rejection within 6 hours of surgery due to pre-existing antibodies. There is complete absence of arterial and venous flow in transplanted kidney on Doppler.

Fig. 10: Afunctional and avascular transplanted right kidney suggestive of hyperacute rejection post transplant.
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694
2. Renal infarction following vascular compromise- detailed under vascular complications.
3. Post-transplant lymphoproliferative disorder (PTLD)- exclusive to transplanted kidney due to oncogenic action of immunosuppressive agents and EBV infection. Presents as perihilar soft tissue thickening,perinephric masses and lymphadenopathy. Reduction in immunosuppressive agents may cause regression of PTLD.
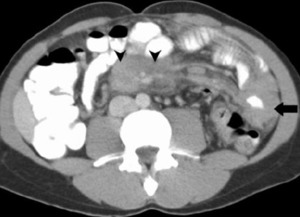
Fig. 11: CECT in post-transplant patient shows encased SMA by lymphadenopathy (arrowheads) and circumferential jejunal wall thickening(arrow)-PTLD
References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356

Fig. 12: CECT in a transplant recipient shows a necrotic mass in pelvis osterior to the transplanted kidney(arrows)-PTLD
References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356
4. Renal cell carcinoma/ Tumours of ureters and urinary bladder- Masses can occur in both native or transplant organs and should be treated accordingly.
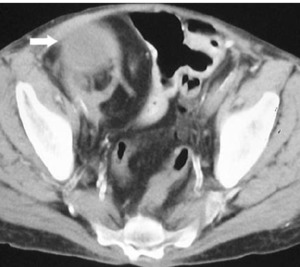
Fig. 13: CECT showing a cystic lesion(arrow) arising from right renal transplant- Renal Cell Carcinoma
References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356
Other renal parenchymal abnormalities like glomerulonephritis,renal abscess,renal cysts etc. appear similar to that in the native kidney.
Delayed graft function due to acute tubular necrosis (ATN),acute rejection, calcineurin inhibitor (CNI) toxicity, BK virus nephropathy,chronic rejection etc. have no specific radiological findings.
Collecting System Complications
1. Hydronephrosis can be non-obstructive(flaccid) due to loss of tonicity from denervation or obstructive due to early postoperative oedema at the ureteral anastomosis or blood clots after surgery and external compression by collections. Delayed obstructive hydronephrosis is caused by ureteral stenosis/fibrosis/ischemia.
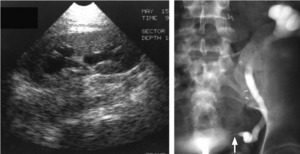
Fig. 14: (A) USG shows mild hydronephrosis which on retrograde pyelogram (B) turns out to be due to narrowing at the site of ureteral implantation into bladder(arrow)-ureteral stricture
References: Choyke PL, Becker JA, Zeissman HA. Imaging the transplanted kidney. In: Pollack HM, McClennan BL, Dyer RB, Kenney PJ, eds. Clinical urography. 2nd ed. Vol 3. Philadelphia, Pa: Saunders, 2000; 3091–3118
RI may be elevated in hydronephrosis. Assessment of exact site and cause of obstructive uropathy is done using non-enhanced CT.
2. Calculus disease- May exist in the donor kidney or develop later. Patient does not experience typical renal colic because the transplanted kidney is denervated.
3. Pyelonephritis/fungal infection- Seen as echogenicity within the collecting system with(out) thickened urothelium.Differntiate from graft rejection and early TCC. MRI urography without contrast maybe used.
4. Urinary leaks due to anastomotic leak.
Perinephric Complications
Early postop fluid collections near kidney are normal and should be followed up for resolution. In all collections, delineate the vessels to rule out leakage or compression of vessel from collection.
1. Urinoma occur around distal ureter,vesico-ureteric anastomosis, cystostomy site and dilated collecting system.On imaging, seen as collections.

Fig. 15: Cystogram demonstrating extravasation(arrow) from ruptured ureterovesical junction stenosis forming a urinoma.
References: Choyke PL, Becker JA, Zeissman HA. Imaging the transplanted kidney. In: Pollack HM, McClennan BL, Dyer RB, Kenney PJ, eds. Clinical urography. 2nd ed. Vol 3. Philadelphia, Pa: Saunders, 2000; 3091–3118
2. Hematoma- Due to graft rupture/leak and can be located perinephrically (‘double contour’ sign on USG) or subcapsularly.

Fig. 16: USG showing subcapsular hematoma- double contour of kidney
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694
3. Lymphocele- Occur few months after surgery due to surgical disruption of lymphatics. Contain chylous fluid and triglycerides. They progressively grow in size (cf. seroma)
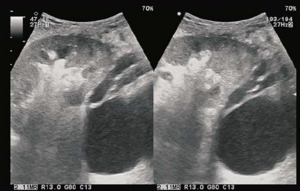
Fig. 17: USG shows a large lymphocele dorsal to the transplant kidney.
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694
4. Seromas- Contain clear fluid and do not grow over time.
5. Abscess- Irregular, dense fluid collections with postcontrast peripheral enhancement.
T2 MRI is very sensitive to presence of a collection. However, it cannot reliably differentiate between them. Before image guided aspiration, rule out aneurysm by doppler as it also appears hypoechoic round mass.
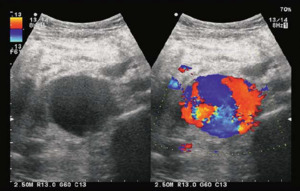
Fig. 18: USG shows a large anechoic lesion imitating lymphocele which takes colour and is aneurysm of transplant renal artery.
References: T2 MRI is very sensitive to presence of a collection. However, it cannot reliably differentiate between them.
Vascular Complications
Contrast is avoided for the fear of worsening renal failure. However, MRA may be employed.
1. Renal artery thrombosis-Early diagnosis and treatment help in allograft salvage. Colour Doppler shows absent flow in transplant renal artery and intra-renal vessels along with an echogenic thrombus within lumen.
2. Renal Infarction- Consequential of rejection, vasculitis or vascular thrombosis. Segmental infarcts appear as ill-defined hypoechoic areas with no vascularity and are caused due to vasculitis.
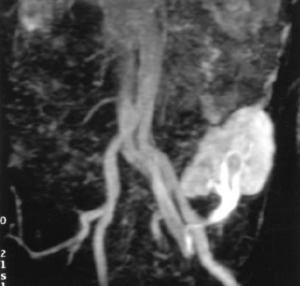
Fig. 19: MIP image demonstrating occlusion of a graft renal artery with lack of perfusion to lower pole causing infarction.
References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356
In complete renal infarct, kidney is oedematous, diffusely enlarged and hypoechoic with absent flow. Tc99 radionuclide scan shows photopenia of the infarct area.
3. Renal vein stenosis/thrombosis - Caused by external compression or extension of iliac vein thrombosis,hypovolemia,dysfunctional anastomosis and slow flow secondary to rejection. Increased prevalence in left lower quadrant allografts attributed to compression of the left common iliac vein between the sacrum and the left common iliac artery (silent iliac artery compression syndrome).
USG demonstrates an enlarged kidney with flow and thrombus. Intrarenal arterial system and the transplant renal artery show increased resistance often resulting in reversed diastolic flow. CECT and MR venography also used.Prompt thrombectomy following early diagnosis can salvage graft.
4. Renal artery stenosis
Doppler parameters for diagnosis include PSV >2 m/s, turbulence distal to that area, and intrarenal parvus-tardus waveform with RI lower than 0.50.
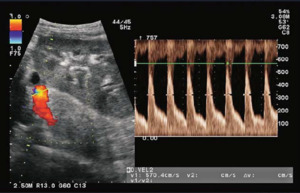
Fig. 21: Color and spectral Doppler show increased flow rate (5.7m/s) in the prehilar segment of renal artery corresponds to stenosis.
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694
The ratio of PSV in the renal artery to PSV in the external iliac artery greater than 3 is also indicative. CT/MRI angiography is used in diffiucult cases.
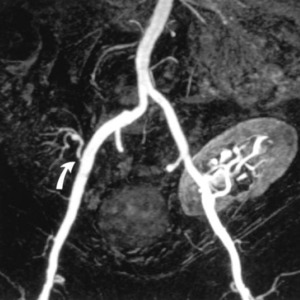
Fig. 20: MIP shows severe proximal stenosis(arrow) in the first renal transplant on right.
References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356
5. Aneurysmal dilatation of the renal arteries Fig. 18 is seen on USG and must be differentiated from dilated pyelon. Doppler waveform o and from pattern). Aneurysms can be poststenotic, mycotic or iatrogenic.
Post-biopsy Complications
1. Arteriovenous Fistulas- AVF form when an artery and vein are lacerated. Spectral Doppler analysis shows PSV >3 m/s. USG shows local areas of disorganized color spilling outside vascular lumen (perifistula vibration).Feeding artery shows high-velocity,low-resistance waveform. Draining vein demonstrates arterialization.

Fig. 22: A.Colour Doppler USG demonstrates a localised area of disorganised colour with high velocity and low impedence waveform (B)- AVF
References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694
2. Pseudoaneurysms- PA results when only the artery is lacerated. Doppler shows elevated PSV>3 m/s with arterialization of venous waveform.
Both PA and AVF resolve spontaneously but regular Doppler follow up is required to assess need for intervention.
Gastrointestinal and Herniation Complications- Postoperative adhesions causing intestinal obstruction, herniation of bowel through peritoneal defect leading to compromise of transplant. Urinary obstruction from obturator herniation of the ureter.
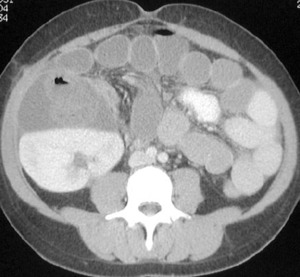
Fig. 23: CECT shows multiple distended small bowel loops around transplanted kidney- compatible with obstruction due to herniation from the peritoneal defect.
References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356

: 1035-1041")
: 165-172.")
: 1035-1041")
: 517-531")
 NECT MIP image in a potntial recipient shows intensive arterial wall calcifications (iliac or splenic anastomosis was not possible). (b, c) Frontal (b) and lateral (c) volume-rendered images show a vascular aortofemoral prosthesis (arrowhead), implanted 2 months before kidney transplantation; correct permeability can be seen. There is early ipsilateral venous enhancement (arrow), which is a normal finding in patients with a vascular aortofemoral prosthesis. Left transplant anatomosis was made with the prosthesis. References: Catalá, Violeta, et al. "Use of multidetector CT in presurgical evaluation of potential kidney transplant recipients." Radiographics 30.2 (2010): 517-531")
: 517-531.")
: 694")
Normal Colour and spectral doppler of the anastomosis of transplant artery on iliac artery (PSV 1.5m/s)
(B) Normal colour and spectral doppler in the renal vein. References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694.")
: 694")
: 694")
 and circumferential jejunal wall thickening(arrow)-PTLD References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356")
-PTLD References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356")
 arising from right renal transplant- Renal Cell Carcinoma References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356")
 USG shows mild hydronephrosis which on retrograde pyelogram (B) turns out to be due to narrowing at the site of ureteral implantation into bladder(arrow)-ureteral stricture References: Choyke PL, Becker JA, Zeissman HA. Imaging the transplanted kidney. In: Pollack HM, McClennan BL, Dyer RB, Kenney PJ, eds. Clinical urography. 2nd ed. Vol 3. Philadelphia, Pa: Saunders, 2000; 3091–3118")
 from ruptured ureterovesical junction stenosis forming a urinoma. References: Choyke PL, Becker JA, Zeissman HA. Imaging the transplanted kidney. In: Pollack HM, McClennan BL, Dyer RB, Kenney PJ, eds. Clinical urography. 2nd ed. Vol 3. Philadelphia, Pa: Saunders, 2000; 3091–3118")
: 694")
: 694")

: 1335-1356")
 in the first renal transplant on right. References: Akbar, Syed A., et al. "Complications of renal transplantation." Radiographics 25.5 (2005): 1335-1356")
 in the prehilar segment of renal artery corresponds to stenosis. References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694")
- AVF References: Sjekavica, Ivica, et al. "Radiological Imaging in Renal Transplantation." Acta Clinica Croatica 57.4 (2018): 694")
: 1335-1356")











