ECR 2020 / C-08490
Comprehensive Review of Cystic Pancreatic Tumors for the Practicing Radiologist
Congress:
ECR 2020
Poster Number:
C-08490
Type:
Educational Exhibit
Keywords:
Not applicable, Cysts, Staging, Contrast agent-intravenous, Biopsy, MR, CT, Pancreas, Abdomen, Abdominal Viscera
Authors:
N. Venugopal1, N. Kinger2, C. Moreno3, M. Roda4, F. H. Miller5, P. Mittal6; 1Duluth/US, 2Atlanta, Georgia/US, 3Atlanta/US, 4Jackson , MS/US, 5Chicago, IL/US, 6Decatur, GA/US
DOI:
10.26044/ecr2020/C-08490

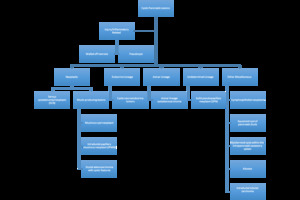
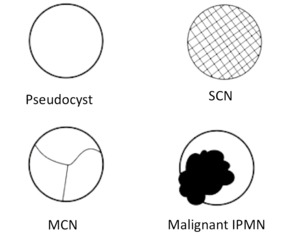
Fig. 2:
Pathologic classification of cystic lesions of the pancreas.
 Pancreatic Pseudocyst: smooth walled cyst with encapsulation of the pancreatic secretions by granulation tissue and a fibrous capsule, (top right) Serous Cystadenoma/Neoplasm: honeycomb appearance (bottom left) Mucinous Cystic Neoplasm: Unilocular or multilocular appearance and (bottom right) Malignant IPMN: Unilocular or cluster of cysts (dilated ducts), lobulated margins.
References: Augusta/US")
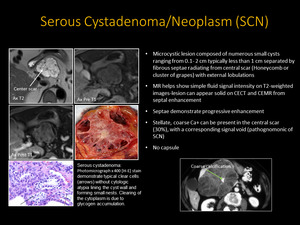
Fig. 3:
Cystic changes characteristic of (top left) Pancreatic Pseudocyst: smooth...
:
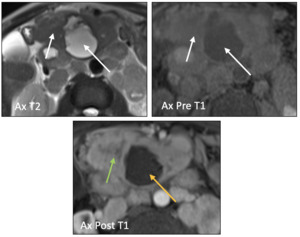
Serous cystadenoma: Axial T2 weighted MR image reveals fibrous septae radiating from a central scar ( white arrows). Coarse calcification visualized within central scar following contrast administration (green arrows). References: Augusta/US")
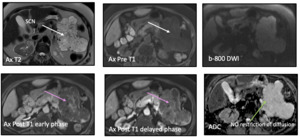
Fig. 4:
Serous Cystadenoma/Neoplasm (SCN):
Serous cystadenoma: Axial T2 weighted MR...
. Progressively enhancing septae following contrast administration (pink arrows). On DWI, mass shows high ADC due to no restriction (green arrow). References: Augusta/US")
Fig. 5:
Serous cystadenoma: 70-year-old female with history abdominal pain. Axial T2...
: Variants
References: Augusta/US")
Fig. 6:
Serous Cystadenoma(SCN): Variants

Fig. 7:
Differential Diagnosis of Oligocystic SCN
: Variants References: Augusta/US")
Fig. 8:
Serous Cystadenoma(SCN): Variants

Demographics and Background
References: Augusta/US")
Fig. 9:
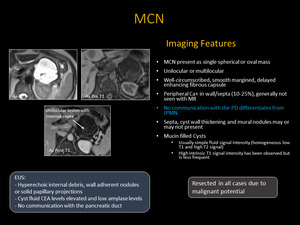
Mucinous Cystic Neoplasm (MCN)
Demographics and Background

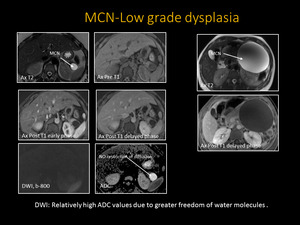
Fig. 10:
MCN
. Axial T1 post-contrast images re-demonstrates the non-enhancing, unilocular lesion. The same mass demonstrates no diffusion restriction and high signal on ADC (arrows). References: Augusta/US")
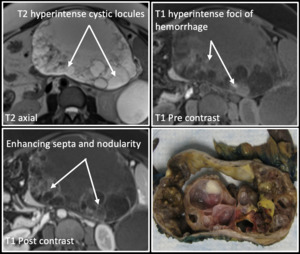
Fig. 11:
Mucinous Cystic Neoplasm: Axial T2 weighted MR image reveals homogenous,...
. Axial T1 images demonstrate hyperintense foci of hemorrhage and septa that enhance with contrast (arrows). A surgically resected specimen demonstrates similar findings. References: Augusta/US")
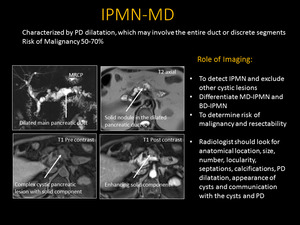
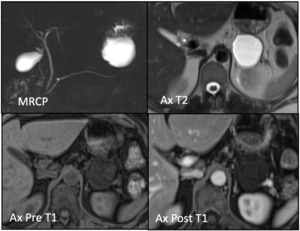
Fig. 12:
Mucinous Cystic Neoplasm with Invasive Adenocarcinoma: Axial T2 weighted MR...
. Axial T1 weighted MR image re-demonstrates complex, cystic pancreatic lesion with a solid component that enhances with contrast. MRCP showing dilation of the main PD (arrows) representing a main duct IPMN. References: Augusta/US")
Fig. 13:
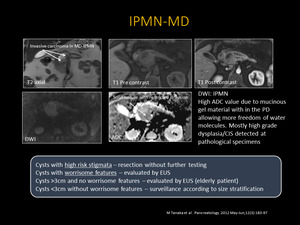
Main Duct Intraductal Papillary Mucinous Neoplasm: Axial T2 weighted MR image...

Fig. 14:
DWI solid pancreatic nodule with diffusion restriction. High ADC value due to...
 with lobulated margins that communicates with the PD, which itself is not dilated (top image) 25-40% of Branch Duct IPMNs are multifocal as seen in the bottom image that demonstrates multiple unilocular lesions communicating with the PD in the absence of pancreatic ductal dilation (bottom image). References: Augusta/US")
Fig. 15:
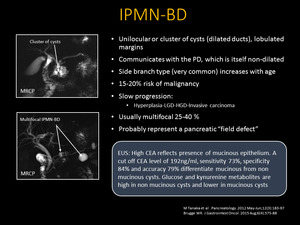
Branch Duct IPMN: MRCP showing a cluster of cysts (dilated ducts) with...

Fig. 16:
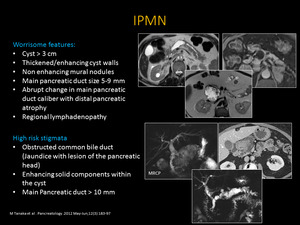
IPMN
Worrisome features and High risk stigmata

Fig. 17:
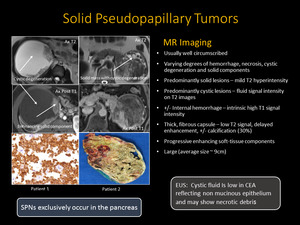
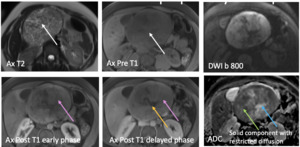
Solid Pseudopapillary Tumors
 with T2 hyperintense areas due to necrosis/cystic degeneration and corresponding precontast T1weighted image shows intermediate signal (black arrow) . Following contrast administration mass show progressive enhancement (pink arrows) with areas of non enhancement due to cystic degeneration (yellow arrow). On DWI, soild portion of the mass shows low ADC due to restriction (green arrow) where as cystic components show high ADC (blue arrow).
References: Augusta/US")
Fig. 18:
Solid pseudopapillary neoplasm: 26 -year- old female with history of abdominal...
, T2 hypointense and intermediate T1 signal thick rind of soft tissue (yellow arrows) that shows enhancement following contrast administration and restricted diffusion due to dark ADC (green arrows) and no enhancement of central aspect due to necrosis (dashed arrow). The mass encases the celiac axis, hepatic artery and splenic artery by 360 degrees (white arrows). References: Augusta/US")
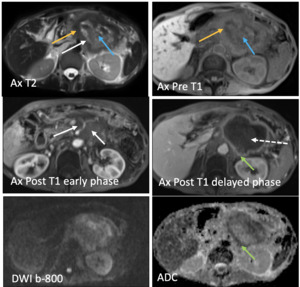
Fig. 19:
Pancreatic adenocarcinoma: 79-year-old female with history left upper quadrant...
 and corresponding precontast T1weighted image shows intermediate signal (white arrow). Following contrast administration, the mass shows heterogenous enhancement (pink arrow) with areas of non enhancement due to cystic degeneration (blue arrow). Photomicrograph x 40 [H-E] stain demonstrate haphazard and infiltrative growth of malignant glands, some glands contain necrotic debris, and a back ground of desmoplastic stroma. Black arrow indicates malignant glands, with necrosis in the center. Red arrow indicates desmoplastic stroma.
References: Augusta/US")
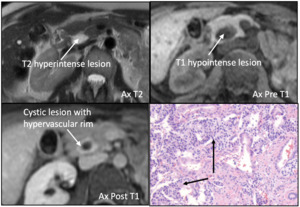
Fig. 20:
Pancreatic adenocarcinoma: 68 -year- old male with history abdominal and back...
. Axial T1 weighted MR also demonstrates a hypervascular rim that enhances with contrast (white arrows).
Photomicrograph x 100 [H-E] stain demonstrates interface between normal pancreas in the lower portion of the slide and neuroendocrine tumor on the top ( black arrows) the tumor cells are forming nests and show monotonous cells with pink granular cytoplasm. References: Augusta/US")
Fig. 21:
Neuroendocrine tumor: Axial T1 and T2 weighted MR images show homogeneously T1...

Fig. 22:
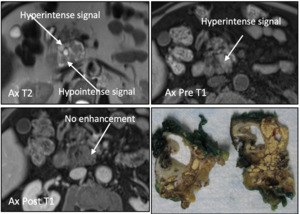
Unilocular Lymphoepithelial Cyst: Axial T2 weight MR image showing T2...
. The same lesion demonstrates T1 hyperintensity without contrast enhancement (arrows). Surigcally resected specimen shows a heterogeneous mass filled with keratinaceous debris.
References: Augusta/US")
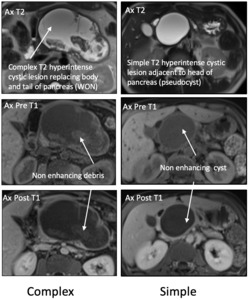
Fig. 23:
Multilocular Lymphoepithelial Cyst: Axial T2 weight MR image showing a...
: Axial T2 weighted MR image showing complex T2 hyperintense cystic lesion replacing the body and tail of the pancreas with T2 hypointense proteinaceous debris (arrow). Axial T1 weighted MR image showing T1 hypointense heterogeneous cystic lesion filled with non-enhancing debris that does not enhance with contrast (arrow).
Simple Pseudocyst (Right): Axial T2 weighted MR image showing homogeneous and well-circumscribed T2 hyperintense cystic lesion. Axial T1 weighted MR image showing homogeneous and well-circumscribed T1 hypointense cystic lesion that does not enhance with contrast (arrows). References: Augusta/US")
Fig. 24:
Complex Walled off Necrosis (Left): Axial T2 weighted MR image showing complex...
, with central T2 hyperintense and T1 hypointense necrosis (black arrows) involving the pancreatic head. Post contrast T1 weighted image shows heterogeneous enhancement of solid mass (green arrow) and no enhancement of central aspect (yellow arrow). Biopsy showed (acinar cell carcinoma.) References: Augusta/US")
Fig. 25:
Acinar Cell Cystadenocarcinoma: 54 -year- old male with history abdominal pain....