Imaging investigation methods
Characterization of ovarian lesions is of great importance in order to plan adequate therapeutic procedures. Optimal assessment of adnexal masses requires a multidisciplinary approach, based on physical examination, laboratory tests and imaging techniques.
1. Ultrasound (US) is often the first imaging study performed in the evaluation of a suspected ovarian lesion because it’s widely available, well accepted by patients, non-invasive and of low cost.
2. Computed Tomography (CT) is the imaging technique of choice in staging and therapy response evaluation.
3. Magnetic Resonance Imaging (MRI) is an essential problem solving tool to determine the site of origin of a pelvic mass and then to characterize an adnexal mass, especially in patients with indeterminate lesions.
Morphological features suggestive of malignancy include:
- thickness (>2–3 mm) and irregularity of walls and septa;
- the presence of solid areas and papillary projections;
- other evidence of malignant activity, namely ascites, peritoneal nodules and metastatic lesion.

Fig. 6: Features that suggest either benign or malignant epithelial neoplasms.
References: https://www.researchgate.net/figure/Features-that-Suggest-Either-Benign-or-Malignant-Epithelial-Neoplasms_tbl3_11035493
Procedure details
We assesed by imaging techniques (US, 8-slice CT scanner and 0,4 T MRI machine) 3 cases of pediatric patients with abdominal palpable mass, abdominal distension and pain, which histopathologically proved to be serous ovarian cystadenoma, mature teratoma and juvenile granulosa cell tumor.
The preferred initial imaging investigation of the patients pelvis was gray-scale ultrasound with additional color Doppler imaging. For further lesion and global assessment of the abdomen and pelvis both CT and MRI imaging evaluation was performed.
Imaging findings from literature data and personal work
Serous ovarian cystadenoma
Epithelial tumors are typically primarily cystic, may be either unilocular or multilocular, and, when malignant, are associated with varying proportions of solid tissue.
The lesion can manifests as:
- a unilocular or multilocular anechoic adnexal lesion with no papillary projections and no flow on color doppler on US;

Fig. 7: 17 years old female with abdominal distension. Ultrasound investigation shows an uniloculated, anechoic, thin-walled cystic-like pelvic mass, with no flow on color Doppler. Because of its size and difficulty in determining origin further imaging investigations were demanded.
- homogeneous CT attenuation or MR imaging signal intensity of the locules, a thin regular wall and no endocystic or exocystic vegetation and no significative contrast enhancement is considered to be a benign serous cystadenoma.

Fig. 8: Serous ovarian cystadenoma in a 17-year-old female.
(Left) Axial nonenhanced CT image shows large homogenous cystic mass (with clear liquid content ~ 17 HU density) arising from pelvis. (Right) Axial enhanced CT image in same patient shows presumably left ovary origin of the mass. (UB-urinary bladder, RO-right ovary)

Fig. 9: Enhanced axial and sagittal CT reconstruction images show poor contrast enhancement within lesion and notable mass effect on the intraabdominal structures (arrows).

Fig. 10: Serous cystadenoma in a 17-year-old female.
(a) Axial and (b) sagittal T2-weighted images show a hyperintense unilocular cystic mass. On (c) axial and (d) coronal T1-weighted images, the cyst has no fat intensity component.
Mature teratoma
Tumors of germ cell origin are the second most common group of ovarian neoplasms, representing 15–20% of all ovarian tumors. Of all the germ cell tumors, only mature teratoma is benign.
US findings in mature cystic teratomas vary from:
- a cystic lesion with a densely echogenic tubercle (Rokitansky nodule) projecting into the cyst lumen;
- diffusely or partially echogenic mass with the echogenic area usually demonstrating sound attenuation owing to sebaceous material and hair within the cyst cavity;
- multiple thin, echogenic bands caused by hair in the cyst cavity.

Fig. 11: 10 years old premenarchal girl with pelvic palpable mass.
Transabdominal ultrasound image depicts a 14 cm right ovarian complex cystic mass with thin, echogenic bands within and mural heterogenous hyperechoic nodule with calcifications and posterior acoustic shadowing, no flow on color Doppler.
At CT, fat attenuation within a cyst, with or without calcification in the wall, is diagnostic for mature cystic teratoma.

Fig. 12: Axial (right) and sagital (left) enhanced CT images in the same patient show right adnexal with abdominal extension of a fluid mass with septa within (arrowhead) and inferior mural nodule (arrows) with soft tissue, fat and calcification HU densities.
MRI usually demonstrates the sebaceous component of dermoid cysts with:
- high signal intensity on T1-weighted similar to that of retroperitoneal fat;
- variable, usually near that of fat signal intensity of the sebaceous component on T2-weighted images;
- a T1-weighted fat-saturated sequence is also able to make differential diagnosis between fat-tissue and haemorrhagic lesions;
- a fat-fluid interface may also be found, and is typical of mature cystic teratoma;
- other features are: areas of low signal intensity (teeth), soft-tissue protuberances (Rokitansky nodules), floating debris.
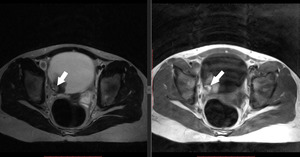
Fig. 13: Mature teratoma in a 10-year-old girl. (Left) Axial T2-weighted image show a well-defined heterogeneous, but predominant T2 hyperintense mass with high signal intensity mural nodule on both T1-weighted and T2-weighted images suggestive for fatty component. A hypointense signal on T2 and T1 is noted within nodule.
Juvenile granulosa cell tumor
Gonadal cell types that derive from sex cords include granulosa cells, theca cells, fibroblasts, Leydig cells, and Sertolicells. Ovarian tumors composed of these cell types are called sex cord–stromal tumors. This group of tumors represents approximately 8% of ovarian neoplasms and affects all age groups.
The most common types are:
- granulosa cell tumors (GCT),
- fibrothecomas, and
- Sertoli-Leydig cell tumors.
Granulosa cell tumours are usually benign; however, they may be malignant as well. Granulosa cell tumours can be divided into two main subtypes, adult and juvenile:
- The adult type is responsible for about 95 % of cases and occurs preferentially in perimenopausal and postmenopausal women.
- The juvenile type is less frequent and affects prepuberal children, leading to pseudoprecocity.
Imaging characteristics of adult and juvenile granulosa cell tumors are non-specific and these tumors cannot be reliably distinguished from other ovarian neoplasms on imaging alone.
1. At ultrasound examination, most GCTs appear as:
- large multilocular–solid masses with a large number of locules, or
- solid tumors with heterogeneous echogenicity of the solid tissue;
- hemorrhagic components are common and increased vascularity is demonstrated at color Doppler ultrasound examination.

Fig. 14: 17 years old juvenile granulosa cell tumor. Ultrasound examination shows large multilocular–solid tumors with heterogeneous echogenicity (white arrows)and internal vascularity (white arrowheads) demonstrated at color Doppler and variable ascitis fluid within peritoneal cavity.
2. On CT imaging their appearance varies widely, but they often appear as:
- a single large multiloculated cystic mass with solid components; they have multiple septations which can be thin, or thick and irregular;
- the adult form shows more variability with regards to the cystic component and can occasionally appear predominantly solid;
- intratumoral hemorrhage, central areas of necrosis and fibrous degeneration can result in a heterogeneous solid appearance.

Fig. 15: Extending superiorly, adjacent to the right ovarian vessels there are lobulated, centrally hypodense masses (asterix) (10x11.5x15 cm ) with further mass more laterally (asterix) (5x4x6 cm) adjacent to the left external iliac vessels with moderate and heterogeneous enhancement following IV contrast, with areas of decrease attenuation within due to necrosis (black arrowheads). Extensive fluid (white arrows) is seen in the peritoneal cavity associated with thickening of the peritoneum which enhances and appears nodular in places (white arrowheads). Subtle thickening/nodularity of the mesentery (white arrowhead).
3. MR imaging is more distinctive. On T2W images, tumors have a sponge-like appearance, indicating alternating solid and cystic spaces. Metastasis, though rare at initial presentation, appear as cystic liver masses or peritoneal implants, similar to epithelial ovarian neoplasms.

Fig. 16: A 17-year-old female histologically proved OGCT in juvenile type. On coronal T2WI image (right), the masses (asyerix) occupy the majority of pelvis with extension into the abdomen. There is cystic areas within tumors (black arrowhead) indicative of central necrosis. (Left) There is omental infiltration (white arrowhead) with diffuse ascites (black arrow) throughout the abdomen and pelvis.



 Axial nonenhanced CT image shows large homogenous cystic mass (with clear liquid content ~ 17 HU density) arising from pelvis. (Right) Axial enhanced CT image in same patient shows presumably left ovary origin of the mass. (UB-urinary bladder, RO-right ovary)")
.")
 Axial and (b) sagittal T2-weighted images show a hyperintense unilocular cystic mass. On (c) axial and (d) coronal T1-weighted images, the cyst has no fat intensity component.")

 and sagital (left) enhanced CT images in the same patient show right adnexal with abdominal extension of a fluid mass with septa within (arrowhead) and inferior mural nodule (arrows) with soft tissue, fat and calcification HU densities.")
 Axial T2-weighted image show a well-defined heterogeneous, but predominant T2 hyperintense mass with high signal intensity mural nodule on both T1-weighted and T2-weighted images suggestive for fatty component. A hypointense signal on T2 and T1 is noted within nodule.")
and internal vascularity (white arrowheads) demonstrated at color Doppler and variable ascitis fluid within peritoneal cavity.")
 (10x11.5x15 cm ) with further mass more laterally (asterix) (5x4x6 cm) adjacent to the left external iliac vessels with moderate and heterogeneous enhancement following IV contrast, with areas of decrease attenuation within due to necrosis (black arrowheads). Extensive fluid (white arrows) is seen in the peritoneal cavity associated with thickening of the peritoneum which enhances and appears nodular in places (white arrowheads). Subtle thickening/nodularity of the mesentery (white arrowhead).")
, the masses (asyerix) occupy the majority of pelvis with extension into the abdomen. There is cystic areas within tumors (black arrowhead) indicative of central necrosis. (Left) There is omental infiltration (white arrowhead) with diffuse ascites (black arrow) throughout the abdomen and pelvis.")