A retrospective study of 10 years including 100 pacients with liver cirrhosis aged 45-80 years underwent abdominal CT and MRI without and with iv contrast injection.
This review illustrates MRI and CT aspects of different benign and malignant hypervascular lesions using protocols as we’ll list bellow.
CT and MRI TECHNIQUE
Multislice CT protocol:
-non-enhanced multi-slice CT;
- contrast enhanced multi-slice CT after injection of 1,5 ml/kc of nonionic iodine based contrast media with a power injector flow of 3,5 mL/s, bolus triger/ROI in the abdominal aorta at the level of celiac trunk (treshold:100UH):
- arterial phase (AP) (30-35 s delayed aquision from the starting point of the injection);
- portal-venous phase (PVP) (70-80 s delayed aquision from the starting point of the injection);
- delayed phase (DP) (150-180 s delayed aquision from the starting point of the injection);
- coronal and sagital MRP reconstructions.
MRI protocol:
- abdominal examination with a 1,5 T MR system with body phased array coils and injection of 0,1 ml/kg gadoxetic acid;
- breath-hold acquisitions contained: three plane localizer, axial T1 Dual Echo, axial T2 FS, T2 coronal with long TE and short TE, DWI, axial 3D T1 FatSat with and without Gd injection in a multiphase aquisition (4 phases-late arterial, venous, transitional); hepatobiliary phase 3D T1 FS was performed 20 minutes after starting the contrast i.v. injection.
CT and MRI TYPICAL ASPECT OF HCC:
- CT: hypodense lesion with marked enhancement in AP and “wash-out” in PVP;
- MRI Fig. 2 : hypointense on T1FS, moderate hyperintense on T2FS, high signal on DWI (increases specificity and sensitivity), arterial hyperenhancement, wash-out on PVP and low signal on HBP.
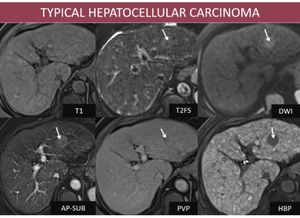
Fig. 2: M, 65yo, HC-HVC. MRI features: nodular lesion in left hepatic lobe isointense with liver parenchima on T1FS, discret high signal on T2, high signal on DWI, hyperenhancing in AP, with “wash-out” in PVP, and hypointense on HBP (arrows);
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania
The imaging features may vary according to it’s histological subtype.
MIMICS of HCC
I.BENIGN LIVER LESIONS
NON-TUMORAL LESIONS
1.Arterio-portal shunts-a communication between a portal venous and an arterial branch secondary to portal hypertension.
Imaging features:
- CT: pseudonodular lesions, usually with peripheral topography, hyperdense on AP and isodense on PVP.
- MRI Fig. 3 : the semiology on the dynamic sequences is identical to that described on CT; note the lesions aren’t visible on other MRI acquisitions.
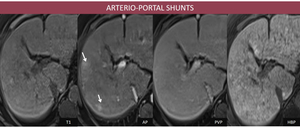
Fig. 3: F, 68yo, HC-HVC. MRI aspects: a few peripheral enhancing foci on AP (arrow), which become isointense to the liver on PVP;
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania
2.Perfusion alteration in portal thrombosis Fig. 4 occurs with venous inflow obstruction and secondary increased arterial flow.
Imaging features:
- CT: spontaneous hypodensity due to edema and transient hight attenuation during the AP and PVP omogenization;
- MRI: in the dynamic sequences, the semiology is identical to that described on CT: low signal on T1FS due to edema or isointense with liver parenchima and transient high attenuation during the AP with PVP isointensity, without correspondent in other aquision.
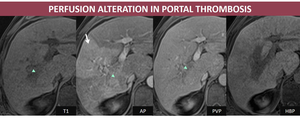
Fig. 4: M, 62yo, HC-HVC. MRI aspects: transient high attenuation in right hepatic lobe (arrow) secondary to portal thrombosis (arrowheads);
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania
TUMORAL LIVER LESIONS
Hemangioma and focal nodular hyperplasia-two rarely encountered lesions in advanced liver cirrhosis and whose diagnosis of certainity is by excluding another tumor origin.
1.Liver hemangioma
Imaging features:
- CT: hypodense lesion on non-enhanced CT with peripheral contrast socket on AP and centripetal and progressive enhancement in late aquisitions;
- MRI Fig. 5: lesion with low signal on T1FS, high signal on T2 FS, high signal on DWI and high signal or isointense on ADC; the semiology on dynamic sequences is identical to that described on CT.
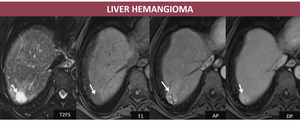
Fig. 5: M, 65yo, HC-HVC. MRI aspects: hepatic subcapsular nodule hyperintense relative to liver parenchyma on T2FS, hypointense relative to liver parenchyma on T1FS, with peripheral enhancement which progress centripetally on delayed images (arrows);
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania
2. Focal nodular hyperplasia Fig. 6
Imaging features:
- CT: often lobulated nodule, hypodense or isodense, hyperenhancing on AP (excepting the central scar which is a common feature) and omogenization on DP. If the central scar is present, it may enhance on DP;
- MRI: isointense/discret low signal on T1FS, isointense/high signal on T2FS acquisition, having the same features on dynamic acquisitions like before described on CT and without restriction on DWI; a particular feature on MRI is lesion’s hyperintensity on HBP when gadoxetic acid is injected.
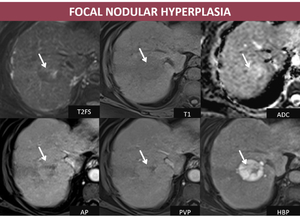
Fig. 6: F, 66yo, HC-HVC. MRI aspects: isointense relative to liver parenchyma on T2FS with hyperintense central scar, hypointense on T1, early arterial enhancement which persist on DP becoming more hyperintense than the background liver on HBP due to abnormal bile ducts (arrows);
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania
II. TUMORAL MALIGNANT LIVER LESIONS
1. Intrahepatic cholangiocarcinoma Fig. 7 is the second most common primary malignancy in a cirrhotic liver. Although the differential diagnostic with HCC is difficult, a few patterns that can guide the diagnosis.
Imaging features:
- CT: hypodense lesion on non-enhanced CT aquisition, usually peripheric, with capsular retraction, peripheral rim enhancement on AP; the central tumoral part show centripetal enhancement on DP;
- MRI: low signal lesion on T1FS with capsular retraction associated, high signal on T2FS, diffusion restriction at high b values; peripheric rim enhancement on AP with late centripetal omogenization (central hypointensity may be represented by fibrosis or necrosis), hypointensity on HBP.
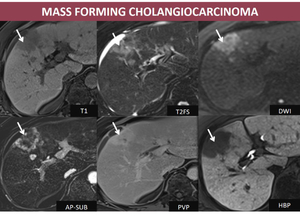
Fig. 7: M, 62 yo, HC-HVC. MRI aspects: peripheric nodule in right hepatic lobe, with low signal on T1, high signal on T2FS, hyperintense on DWI sequence, peripheral progressive enhancement and hypointensity on HBP (arrows); note the hepatic capsular retraction;
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania
2. Biphenotypic tumor Fig. 8 : Combined hepatocellular carcinoma is a rare primary liver tumor on which are encountered both hepatocellular carcinoma and cholangiocarcinoma with a varied pattern of enhancement, depending on the predominance of the cellular type (6).
Imaging features:
- CT: hypodense, with heterogeneous progressive enhancement and/or wash-out if hepatocellular phenotype is dominant;
- MRI: low signal on T1 FS, heterogeneous high signal on T2FS, hyperintese on DWI, progressive peripheral enhancement and HBP hypointensity.
3. Metastases from hypervascular tumors (renal carcinoma, neuroendocrine tumor, melanoma) in a cirrhotic liver are less common than in unaffected liver most probably due to the fact that patients with cirrhotic livers may represent an unfavorable site for metastatic growth (8).
Imaging features:
- CT Fig. 9 : hypodense, intense enhancing in AP with “wash-out” in late acquisitions;
- MRI: low signal on T1FS, high signal on T2FS, with restricted diffusion, and identical behavior with CT on dynamic acquisitions, hypointense on HBP.
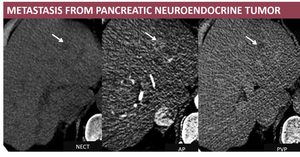
Fig. 9: M, 75 yo, HC-HVB. CT aspects: hypodense nodule, enhancing on AP and “wash-out” on PVP (arrows). Hystopathological exam: neuroendocrine metastasis;
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania

;
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")
, which become isointense to the liver on PVP;
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")
 secondary to portal thrombosis (arrowheads); References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")
; References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")
;
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")
; note the hepatic capsular retraction;
References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")
; References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")
. Hystopathological exam: neuroendocrine metastasis; References: Department of Radiology, Medical Imaging and Interventional Radiology, Fundeni Clinical Institute, Bucharest, Romania")