ECR 2020 / C-11893
A pattern approach to toxic and metabolic encephalopathies: From topographical distribution of affected areas to diagnosis
Congress:
ECR 2020
Poster Number:
C-11893
Type:
Educational Exhibit
Keywords:
Not applicable, Toxicity, Metabolic disorders, Drugs / Reactions, Imaging sequences, MR, Neuroradiology brain, CNS, Neuro
Authors:
P. Guadalupi1, L. milonia1, A. Marrazzo1, C. Giordano2, F. Magnani3, A. Botto2, T. Tartaglione1, S. Gaudino2, C. Colosimo2; 1Roma/IT, 2Rome/IT, 3Roma, Ragusa (RG)/IT
DOI:
10.26044/ecr2020/C-11893

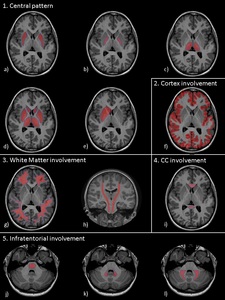
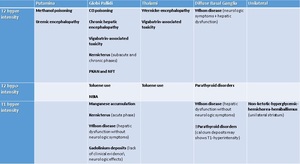
Table 3
 Putamina; b) Globi-Pallidi; c )Thalami; d) Diffuse Basal-Ganglia involvement; e) Unilateral exceptions; f) Cortex involvement; g) Periventricular White-Matter; h) Cortical-spinal tracts; i) Corpus-Callosum; j) Brain stem; k) Dentate-Nuclei; l) Butterfly-wing pattern")
Fig. 1:
a) Putamina; b) Globi-Pallidi; c )Thalami; d) Diffuse Basal-Ganglia...

Table 4
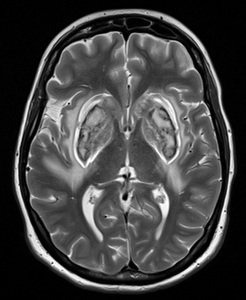
. Bilateral symmetrical signal alteration of the BG: mainly the putamen. a) Bright T2 signal; b) CE in this case; c) SWI: necrotic hemorrhage; d) Restricted diffusion. References: Case courtesy of Dr Annibale Botto, UOC di Neuroradiologia - AOU S. Giovanni di Dio e Ruggi d’Aragona - Salerno/IT")
Fig. 2:
Methanol poisoning caused by accidental ingestion of methanol-containing agents...
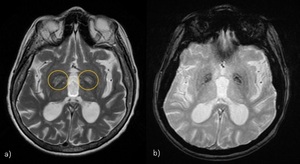
 Simmetric hiperintensities in globi pallidi on T2-WI; b) ADC-map: restricted diffusion. References: Case courtesy of Dr A Mehmet, Radiopaedia.org. From the case rID: 15968")
Fig. 3:
CO poisoning. a) Simmetric hiperintensities in globi pallidi on T2-WI; b)...
.")
Fig. 4:
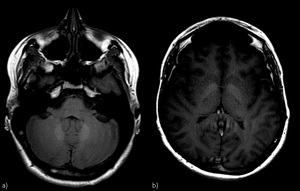
Manganese accumulation. It occurs in chronic hepatic encephalopathy or caused...
. T2-WI hyperintensities in both Globi Pallidi (subacute and chronic phases). They appears hyperintense in T1-WI in the acute phase.")
Fig. 5:
Kernicterus (Bilirubin Encephalopathy in the newborn). T2-WI hyperintensities...
: autosomal dominant form of adult onset NBIA (symptoms: dystonia–chorea and dementia). a)T2-WI: "eye of the tiger" sign: the “eye” corresponds to a region of rarefaction surrounded by more preserved iron-laden neuropil, neurons, and astrocytes; b) SWI: paramagnetic effect of iron deposits.")
Fig. 6:
NBIA, Neuroferritinopathy (NFT): autosomal dominant form of adult onset NBIA...
. Kumar et al. described the elements of the lentiform fork: 1) Lateral arm: edematous external capsule (from the anterior end of the putamen to the stem); 2) Stem: blending of edematous external and internal capsules at the infero-posterior end of the putamen; 3) Medial arm: from the stem to one third of the medial edge where it split into two hyperintense branches engulfing the globus pallidus.")
Fig. 7:
Lentiform fork sign (on T2-WI). Kumar et al. described the elements of the...
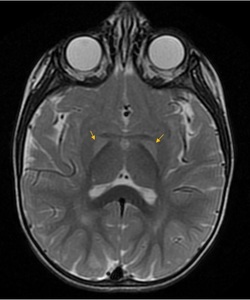
. a)T2-WI show bilateral involvement of the thalami, mammillary bodies (arrows), hypothalamus and periaqueductal GM. Also tectal plate and perirolandic cortex can be affected; b) restricted diffusion; c) CE of mammillary bodies in 80% of cases (pathognomonic). WE is related to chronic alcohol abuse, but also to all the conditions that lead to malnutrition and thiamine deficiency (e.g. hyperemesis, bariatric surgery), an important vitamin (B1) involved in cell membrane integrity.")
Fig. 8:
Wernicke-encephalopathy (WE). a)T2-WI show bilateral involvement of the...
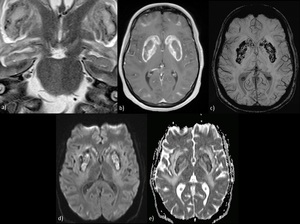
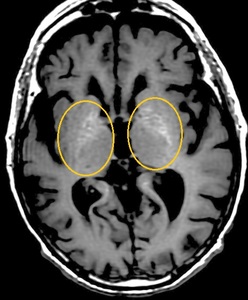
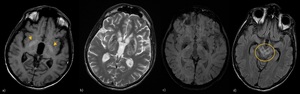
 in two different patients. a) Patient 1, Wilson disease with hepatic dysfunction without neurologic symptoms: T1-WI show hyperintesities of Globi Pallidi; b,c,d) Patient 2, Wilson disease with simultaneous neurologic symptoms and hepatic dysfunction: (b) symmetrical increased T2 signal in the basal ganglia (ventro-lateral thalami involvement can be present);(c) hypointense deposits on SWI in WD patients are mainly caused by iron deposition (Yang J. et al); (d) “Face of the Giant Panda” sign: T2-hyperintensity of the midbrain excluding the red nuclei (eyes) and lateral pars reticulata of the substantia nigra (ears) which are hypointense.")
Fig. 9:
Wilson disease (WD) in two different patients. a) Patient 1, Wilson disease...
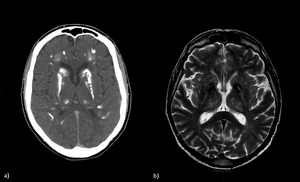
 Patients with Fahr's Syndrome (rare, genetically dominant condition): TC shows the idiopathic iperdense calcifications in basal ganglia; b) Patient with hypoparathyroidism: T2-WI shows bilateral hypointensities (calcium deposits) involving the basal ganglia.")
Fig. 10:
a) Patients with Fahr's Syndrome (rare, genetically dominant condition): TC...
 - Extrapontine myelinolysis. Axial T2\FLAIR images shows diffuse Basal ganglia involvement (symmetric and bilateral hyperintensities) and juxtacortical hyperintense lesions (arrows). Cortex can be also involved in extrapontine myelinolysis.")
Fig. 11:
Osmotic Demyelination Syndrome (ODS) - Extrapontine myelinolysis. Axial...
 or diabetic striatopathy. T1-WI shows hyperintensity of the right lentiform and caudate nuclei. No mass effects. Chorea and ballismus develops rapidly during episodes of non-ketotic hyperglycemia (> in type 2 diabetes mellitus). Symptoms resolve after normalization of glucose levels. References: Case courtesy of Dr Ayaz Hidayatov, Radiopaedia.org. From the case rID: 56241")
Fig. 12:
Non-ketotic hyperglycemic hemichorea (NHH) or diabetic striatopathy. T1-WI...
 Symmetric T2\FLAIR hyperintensities and restricted diffusion (c) in the insular and cingulate gyri. Also basal ganglia and thalami can be involved.")
Fig. 13:
Hyperammonemia. a, b) Symmetric T2\FLAIR hyperintensities and restricted...
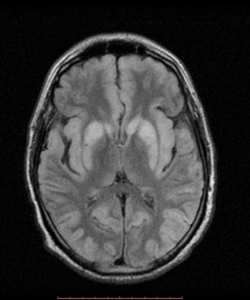
 FLAIR axial image shows symmetric hyperintensities in the parieto-occipital and temporal regions. Basal ganglia are also involved, thalami are spared. Lesions also present Restricted diffusion. References: Case courtesy of Dr Nikos Karapasias, Radiopaedia.org. From the case rID: 25687")
Fig. 14:
Hypoglycemic brain injury (in adults) FLAIR axial image shows symmetric...
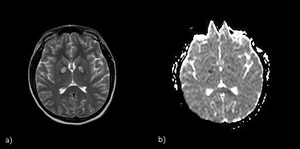
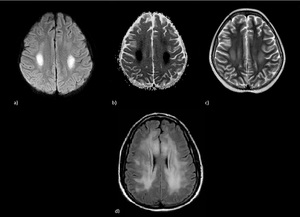
 Patient 1: Bilaterally hyperintensities on T2-WI in the centrum semiovale with diffusion restriction; d) Patient 2: bilaterally asymmetric (across multiple vascular territories) high T2 signal alterations of the deep white matter, subcortical U-fibers are spared. References: Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org. From the case rID: 27698 and Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org. From the case rID: 4438")
Fig. 15:
Methotrexate leukoencephalopathy: a, b, c) Patient 1: Bilaterally...
. Axial T2-WI show confluent, bilateral and symmetric hyperintensities involving posterior limb of internal capsule, perirolandic subcortical white matter, occipital lobes and also the cerebellar white matter sparing the dentate nuclei (butterfly-wing pattern). The anterior limb of the internal capsule and subcortical U-fibers are usually spared. Restricted diffusion is usually present in the acute phase. References: Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org. From the case rID: 4442")
Fig. 16:
Inhaled Heroin (chasing the dragon). Axial T2-WI show confluent, bilateral and...
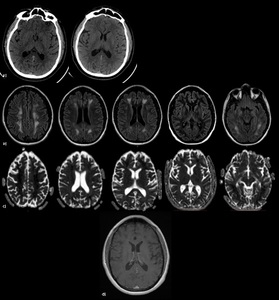
 after Benzodiazepine overdose - The pathomechanism of DPHL is not fully understood (myelin-sheath damage?). DPHL is mainly described in the context of CO intoxication and other causes of hypoxia (drug overuse, cardiac arrest, strangling, seizures). a) Unenhanced CT images of a patient found comatose at home show symmetrical and bilateral hypointensities of the globus pallidus, no involvement of withe matter. After few days the patient clinically improved and was extubated; b, c, d)MRI after 4 weeks show symmetric T2-hyperintensities (b) of the white matter with a marked diffusion restriction (c) and no contrast-enhacement (d). The cortex, U-fibers and infratentorial structures are spared.")
Fig. 17:
Delayed Post-hypoxic Leukoencephalopathy (DPHL) after Benzodiazepine overdose -...
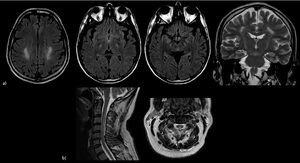
 deficiency. a) Intracranial findings: axial and coronal T2\FLAIR images show bilateral hyperintensities of the corticospinal tracts; b) Medullary findings: dorsal and lateral spinal cord columns are affected (inverted V-shape sign in axia image). Usually there is a complete resolution after treatment.")
Fig. 18:
Cobalamin (B12) deficiency. a) Intracranial findings: axial and coronal...
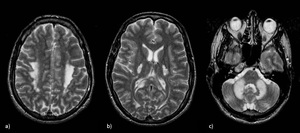
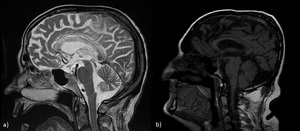
. Related to chronic ethanol abuse: osmotic demyelination and necrosis of the corpus callosum. a) Patient 1: sagittal T2-WI show hyperintensities in the corpus callosum ; b) Patient 2: sagittal T1-WI show selective involvement (hypointensities) of the middle layers of the corpus callosum (sandwich sign).
In the chronic MBD, the CC appears thinner.")
Fig. 19:
Marchiafava-Bignami disease (MBD). Related to chronic ethanol abuse: osmotic...
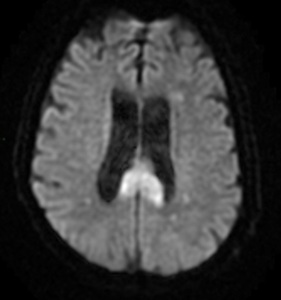
. Oval lesion with restricted diffusion in the splenium. CLOOCs are associated with drug therapy, malignancy, infections, subarachnoid hemorrhage, metabolic abnormalities, trauma and represent an important imaging differential diagnosis for MBD. Typically shows one of three patterns: 1) a small round or oval lesion in the center of the splenium, 2) a lesion centered in the splenium but extending through the callosal fibers, 3) a lesion centered in the posterior portion of CC but extending anteriorly. They are usually reversible probably due to excitotoxic intracellular and/or intramyelinic edema.")
Fig. 20:
Cytotoxic Lesions Of the Corpus-Callosum (CLOCCs). Oval lesion with restricted...
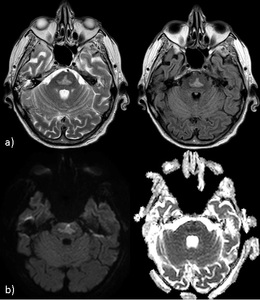
 T2\FLAIR axial images and b) DWI and ADC-map show well-demarcated trident-shaped lesion on the central pons (sparing the periphery); restricted diffusion appears 24 hours after the onset of Osmotic Demyelination Syndrome (oligodendrocytes of the pons are more vulnerable to osmotic changes).")
Fig. 21:
Pontine myelinolysis. a) T2\FLAIR axial images and b) DWI and ADC-map show...
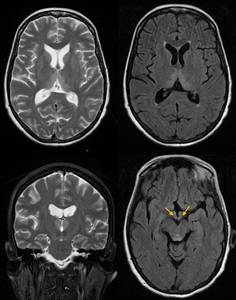
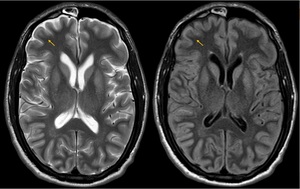
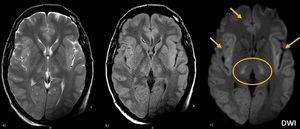
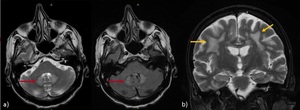
 Axial T2\FLAIR images (red arrows) show symmetric hyperintensities of dentate nuclei (without CE); b) Coronal T2-WI (yellow arrows) shows involvement of periventricular white matter. The splenium can be also involved.")
Fig. 22:
Metronidazole associated toxicity. a) Axial T2\FLAIR images (red arrows) show...
 T1-WI hyperintensities of dentate nuclei; b) also globi pallidi are involved.
Lack of clinical evidence\neurologic effects of gadolinium deposition.")
Fig. 23:
Gadolinium deposits. a) T1-WI hyperintensities of dentate nuclei; b) also globi...

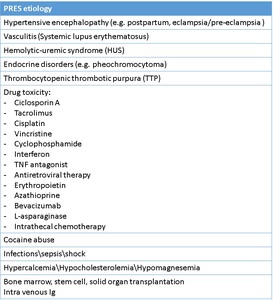
Table 5

Table 6
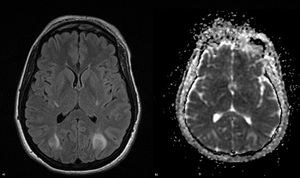
 FLAIR; b) ADC-map. Imaging findings: bilateral, asymmetric hyperintensities on T2-WI\FLAIR involving the subcortical White Matter. ADC-maps are often negative (vasogenic edema). Patchy or variable CE. SWI may show microhemorrhages.")
Fig. 24:
Typical PRES. a) FLAIR; b) ADC-map. Imaging findings: bilateral, asymmetric...

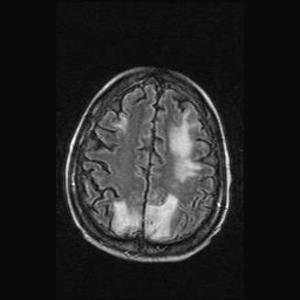
Fig. 25:
Atypical PRES. FLAIR: Superior frontal involvement

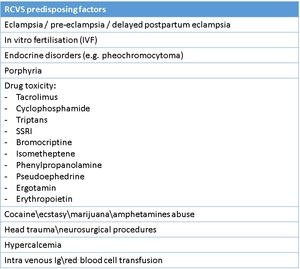
Table 7
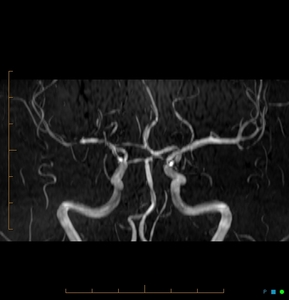
 References: Case courtesy of Dr Chris O'Donnell, Radiopaedia.org. From the case rID: 43356")
Fig. 26:
RCVS. Coronal MRA shows mutiple sites of arterial narrowing (> right side, MCA)