ECR 2020 / C-12283
Uninvited cohabitants: imaging in parasitic diseases
Congress:
ECR 2020
Poster Number:
C-12283
Type:
Educational Exhibit
Keywords:
Abdominal Viscera, Abdomen, CNS, Musculoskeletal soft tissue, CT, MR, Ultrasound, Contrast agent-intravenous, Parasites, Tropical diseases, Retrospective, Not applicable
Authors:
R. HASSAN1, P. P. WALI2, R. V. Helavar1, S. Gopalan1, F. SHAFI3, B. Singh1, S. Kote1, S. B. RAJU1, W. jose2; 1Bangalore/IN, 2BANGALORE, KARNATAKA/IN, 3Bengaluru/IN
DOI:
10.26044/ecr2020/C-12283

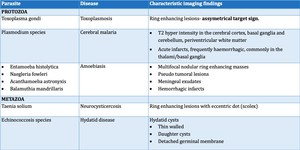
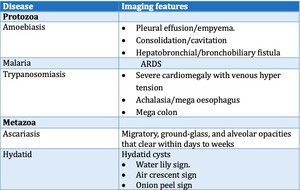
Fig. 2:
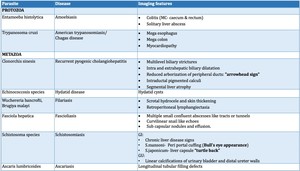
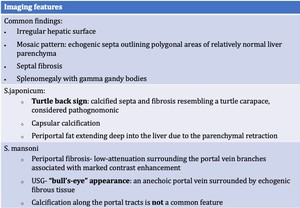
Parasitic diseases of abdomen with salient imaging features

Fig. 3:
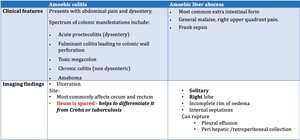
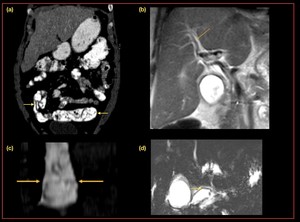
Clinical and imaging features of Amoebiasis
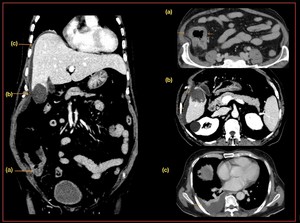
 and adjacent fat stranding in the caecum
b-Ruptured liver abscess with peri hepatic collection
c-Extension of abscess into pleural space with mild right pleural effusion and sub segmental collapse of basal segments.")
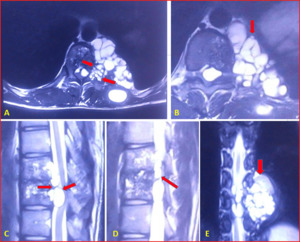
Fig. 4:
Amoebic colitis with ruptured amoebic liver abscess.
Coronal and axial CT...
. [Internet]. Semanticscholar.org. 2020 [cited 14 January 2020]. Available from: https://www.semanticscholar.org/paper/Immunology-of-cystic-echinococcosis-(hydatid-D%C3%ADaz/2f1b2d733f4461d6301efda59d922675c9c62abb/figure/0")
Fig. 5:
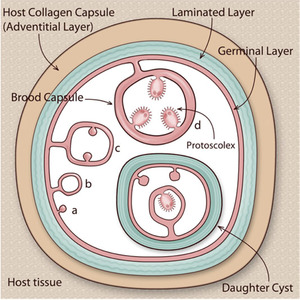
Layers of hydatid cyst

Fig. 6:
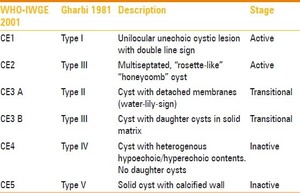
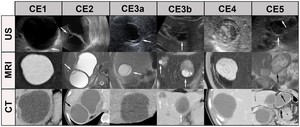
Classification of hydatid cysts

Fig. 7:
Classification of hydatid cysts
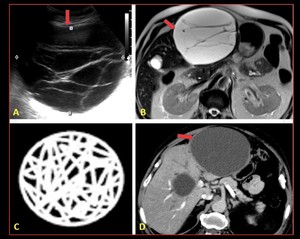
 USG image, (B) axial T2 MRI (C) representative pic (D) Axial CT demonstrating cyst with a predominantly thick membranes.")
Fig. 8:
Hydatidosis : (A) USG image, (B) axial T2 MRI (C) representative pic (D) Axial...

Fig. 9:
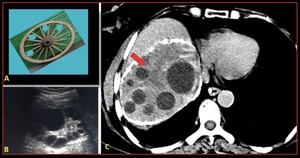
Hepatic hydatid with cart wheel like appearance. Axial CT scan of liver and USG...
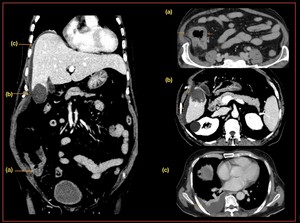
 left kidney, (b) right adrenal gland, (c) intraperitoneal hydatid cyst, axial T2w MRI demonstrates (d) hepatic hydatid cyst")
Fig. 10:
Hydatidosis: Axial CT scan demonstrates, hydatid cyst in the (a) left kidney,...
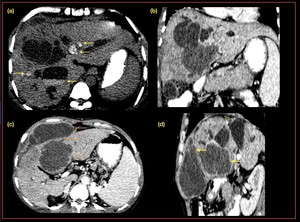
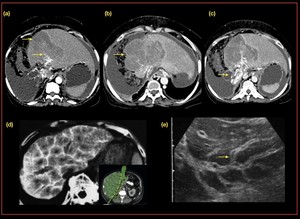
Representative image demonstrating infestation of Clonorchis sinesis causing biliary duct strictures with calculi (b) Axial T2w MRI demonstrating, strictural narrowing of the extra hepatic biliary tree at porta hepatis (orange arrow), multifocal short segment intrahepatic biliary strictures with proximal intrahepatic biliary dilatation (blue arrow), arrow head sign (red arrow),(c) axial CT demonstrates, complete atrophy of segments II, III, IV b and near complete atrophy of segment IV a of left lobe of the liver with thinning and attenuation of the left portal vein, (d)dilated biliary duct/ biliary diverticulum with dependent calculi seen along the anterior border of the caudate lobe")
Fig. 11:
Recurrent pyogenic cholangiohepatitis : (a)Representative image demonstrating...
,(b) Axial CT demonstrates, asymmetrical saccular and fusiform dilatation of the intrahepatic biliary radicles, predominantly in the right lobe of liver with calcific densities within, (c), (d) Cholangitis abscess with rupture and adjacent encapsulated peri hepatic collection.")
Fig. 12:
A case of Recurrent pyogenic cholangiohepatitis with cholangitis and ruptured...
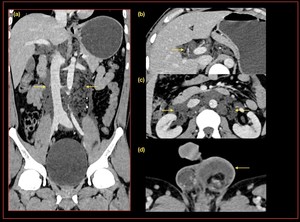
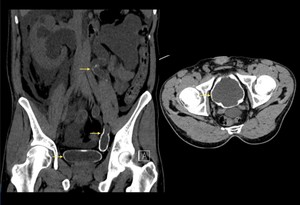
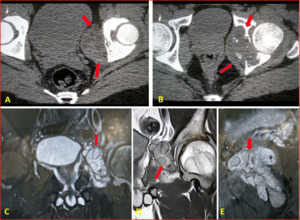
 retro peritoneal lymphangiectasia, which is insinuating into the porta hepatis (a), renal hilum (c) without any mass effect/ infiltration,(d) scrotal hydrocele and skin thickening.")
Fig. 14:
A case of filariasis. Coronal and axial CT demonstrating, (a) retro peritoneal...
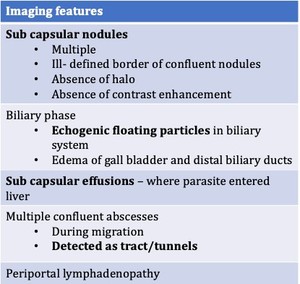
 USG demonstrates, irregular tubular serpiginous hypo echoiec structures in segment V n VIII of right lobe of liver (b) Sagittal CT demonstrates,confluent abscess detected as tract, (c) Axial CT demonstrates, sub capsular and parenchymal hypodense,non enhancing nodules")
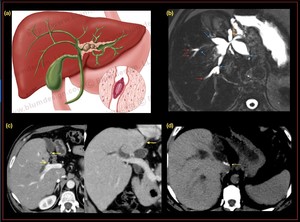
Fig. 16:
Case of hepatic fascioliasis, (a) USG demonstrates, irregular tubular...
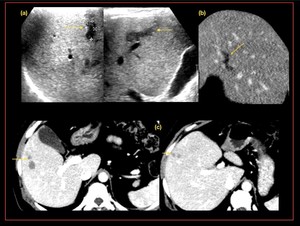
(b)(c)
-Significant atrophy of the right lobe of the liver with hypertrophy of the lateral segment of the left lobe of the liver
-Hypodense poorly enhancing area involving the residual right lobe, caudate lobe and medial segment of left lobe extending into the lateral segment of left lobe and the hepatic hilum.
-Multiple parenchymal calcifications, linear vascular areas of calcification, calcification around porta tracts.
-(d) Turtle back sign
-(e)Peri portal fibrosis (bull’s eye appearance)")
Fig. 18:
Schistostomiasis- Axial CT demonstrates, (a)(b)(c)
-Significant atrophy of...
 Extensive calcification of the urinary bladder and proximal ureter wall, with marked tortuous hydroureters and hydronephyrosis more at the left. References: https://radiopaedia.org/cases/schistosomiasis")
Fig. 19:
Genito urinary Schistostomiasis, Coronal and axial CT demonstrates, (a)...
 and (c) Coronal CT images with oral contrats demonstrating, gastro intestinal ascariasis, (b) and (c) MRCP images demonstrating,biliary ascariasis.")
Fig. 20:
Ascariais- adult worms can be seen as longitudinal tubular filling...
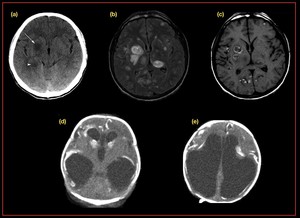
 Axial CT,FLAIR and post contrast images demonstrate show hypodense, hyperintense, ring enhancing lesions in the basal ganglia and left thalamus. Numerous hyperintense lesions also are seen around the gray matter–white matter junctions, findings indicative of a hematogenously disseminated process.
(d,e) CT shows markedly dilated lateral and third ventricles with ventricular wall calcification,severe cortical thinning with multiple parenchymal and deep nuclear calcifications along with the ventricular wall calcifications
References: https://pubs.rsna.org/doi/full/10.1148/rg.294085205, https://radiologykey.com/infection-and-inflammatory-diseases-of-the-central-nervous-system/")
Fig. 23:
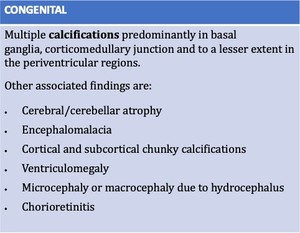
Congenital toxoplasmosis:
(a, b,c) Axial CT,FLAIR and post contrast images...

There are multiple T1 and T2/FLAIR heterogenous lesions with significant peri lesional edema, of varying sizes seen in bilateral cerebral hemispheres, right thalamocapular region, right cerebral peduncle, superior vermis and right inferior cerebellum.
(d)Target sign with multiple concentric T2 hypo intense rings.")
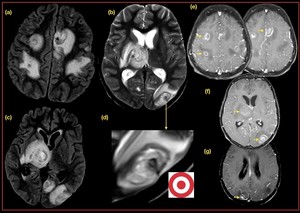
Fig. 25:
Acquired toxoplasmosis: (a,b,c,d,e,f,g)
There are multiple T1 and T2/FLAIR...

Fig. 26:
Cerebral toxoplasmosis with ring enhancing lesions in bilateral basal ganglia
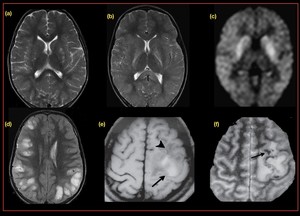
 demonstrate, T2 hyper intense lesion in bilateral basal ganglia which demonstrates diffusion restriction.
(d) Patchy areas of cortical T2 hyper intensity.
Another case of cerebral malaria (e, f), Axial T1W image demonstrates a T1w image demonstrates, hyper intense signal (arrow) in the high left frontoparietal region with surrounding hypo intensity (arrowhead). The gradient image shows blooming (arrow) within the T1 hyperintense area References: https://www.semanticscholar.org/paper/Acute-brain-MRI-findings-in-120-Malawian-children-Potchen-Kampondeni/23d5b203af973473c8bc7e1bc292d5a3c7d06885/figure/1, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2747424/")
Fig. 28:
Cerebral malaria- Axial T2 FSE image (a,b,c) demonstrate, T2 hyper intense...

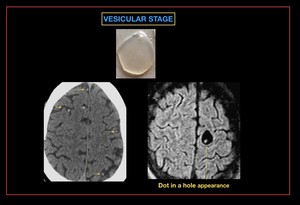
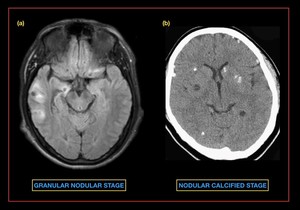
Fig. 31:
Neurocysticercosis- VESICULAR stage

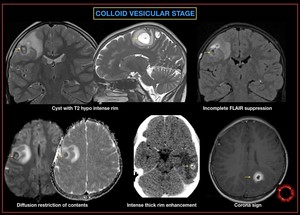
Fig. 32:
Neurocysticercosis- Colloid vesicular stage
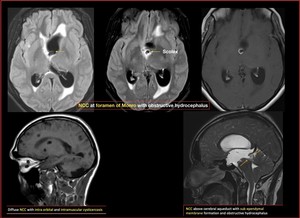
Nodular-granular stage neurocysticercosis - Axial flair image demonstrates, shrinking cysts with minimum mass effect and surrounding gliosis. (b) Calcified granulomas. References: https://www.sciencedirect.com/science/article/pii/S2352621115000030")
Fig. 33:
(a)Nodular-granular stage neurocysticercosis - Axial flair image demonstrates,...

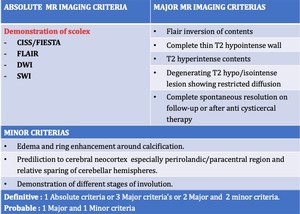
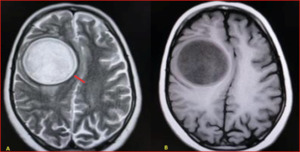
Fig. 34:
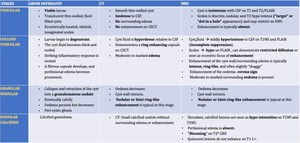
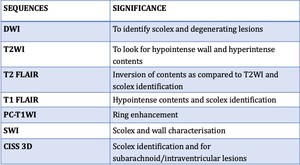
Neurocysticercosis

Fig. 36:
Cerebral hydatid cysts

Fig. 37:
Spinal hydatid cysts

Fig. 38:
Spinal hydatid cysts
 and adjacent fat stranding in the caecum b-Ruptured liver abscess with peri hepatic collection c-Extension of abscess into pleural space with mild right pleural effusion and sub segmental collapse of basal segments.")
Fig. 40:
Amoebic colitis with ruptured amoebic liver abscess. Coronal and axial CT scan...
 : Non contrast axial CT demonstrates, loculated pleural effusion. The axial section of the abdomen demonstrates hypodense lesion lesion contigous with the pleural effusion.")
Fig. 41:
Ruptured amoebic abscess with loculated pleural effusion (possibly empyema) :...

Fig. 42:
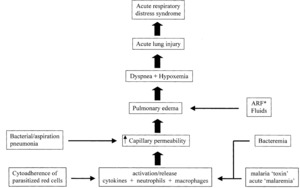
Pathogenisis

Fig. 43:
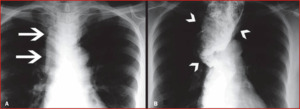
A case of malaria in acute respiratory distress syndrome. Chest radiograph...
. B: Barium swallow examination demonstrating a dilated and tortuous esophagus (arrowheads) References: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0100-39842016000600358")
Fig. 44:
Grade IV megaesophagus. A: Posteroanterior X-ray showing widening of the...

Fig. 45:
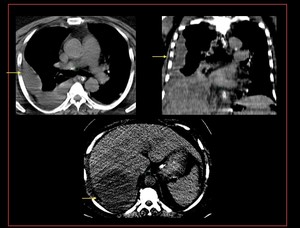
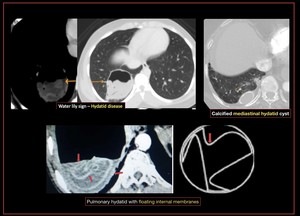
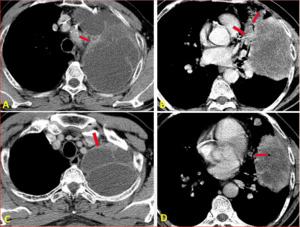
Pulmonary hydatid cysts
, Image D showing air within cyst secondary to bronchial communication")
Fig. 46:
Pulmonary hydatid with intrabronchial communication (A,B,C), Image D showing...
 Chest radiograph shows areas of ground-glass increased opacity in the right lower and middle lobes. (b) High-resolution CT scan shows areas of ground-glass attenuation that correspond to the findings in a. The resolution of radiologic findings 1 week later demonstrated the transient nature of the disease. Larvae and eggs of A lumbricoides were found at bronchoalveolar lavage and in a fecal smear, respectively, during the acute stage. References: https://pubs.rsna.org/doi/full/10.1148/rg.251045043#F14A")
Fig. 47:
Ascariasis in a 35-year-old man with migratory infiltrates. (a) Chest...
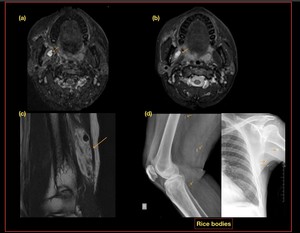
 T2 hyper intense cystic lesion with eccentric nodule.
(c) Myocysticercosis in the triceps muscle (d) Rice bodies")
Fig. 48:
Myocysticercosis
(a,b) T2 hyper intense cystic lesion with eccentric nodule....
 MRI images in same patient demonstrates Cystic lesion with daughter cysts within suggestive of bony hydatid cyst")
Fig. 49:
Bone hydatid cyst: Axial CT scans demonstrates partial destruction of the...
/nodal calcification.")
Fig. 50:
Calcifications seen in the right axilla and in the right infraclavicular region...