ECR 2020 / C-12436
Abdominal wall endometriosis: thinking outside the box
Congress:
ECR 2020
Poster Number:
C-12436
Type:
Educational Exhibit
Keywords:
Not applicable, Tissue characterisation, Hernia, Surgery, Education, Complications, Ultrasound, MR, CT, Musculoskeletal soft tissue, Genital / Reproductive system female, Abdomen, Genitourinary
Authors:
C. D. O. Mira1, A. Guerra2; 1Loures/PT, 2Lisboa/PT
DOI:
10.26044/ecr2020/C-12436

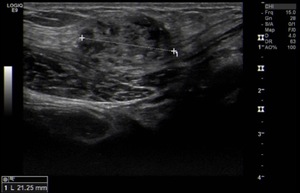
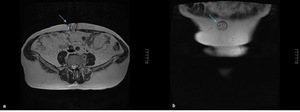
Fig. 1:
Anterior abdominal wall solid lesion in a 29-year-old woman with a history of...

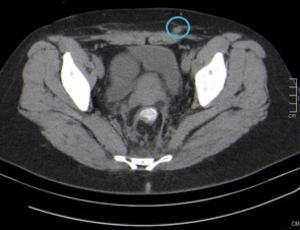
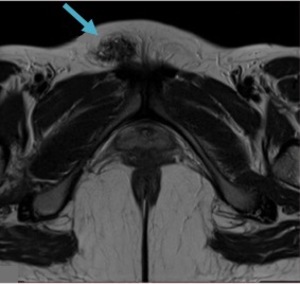
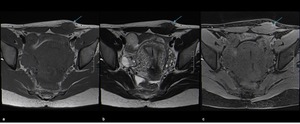
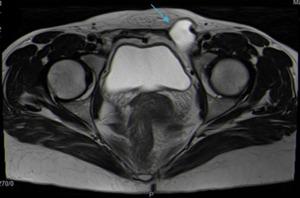
Fig. 2:
Anterior abdominal wall solid lesion in a 34-year-old woman with a previous...
, T2WI (b) and T1 FSWI (c) showing a nodule (blue arrow) displaying the “shading sign”, with high signal on T1WI and T1 FSWI and lower signal on T2WI.
References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
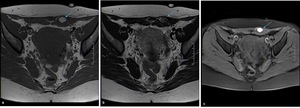
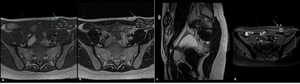
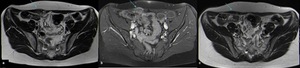
Fig. 3:
Anterior abdominal wall endometriotic implant in a 32-year-old woman with a...
, axial T2WI (b), sagittal T2WI (c) and T1 FSWI (d) showing a spiculated nodule (blue arrow) displaying isointensity relative to muscle on T1WI and T1 FSWI and also low signal intensity on T2WI, consistent with chronic scar endometriosis. References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
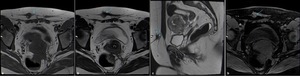
Fig. 4:
Anterior abdominal wall endometriotic implant in a 36-year-old woman with a...
.
References: Catarina Mira/ Lisboa 2019")
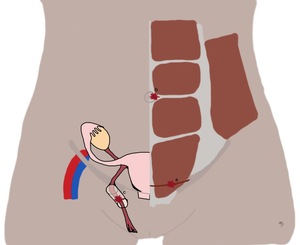
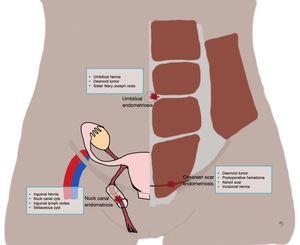
Fig. 5:
Drawing of the female abdominal wall showing the most common locations of...
, axial T2WI (b), sagittal T2WI (c) and T1 FSWI (d) showing a nodule (blue arrow) with hyperintense foci on both T1WI and T2WI consistent with an endometriotic implant.
References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
Fig. 6:
Anterior abdominal wall endometriotic implant in the left rectus abdominis...
. At surgery it proved to be an endometriotic implant. References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
Fig. 7:
Prepubic endometriotic implant on the pubic area of a 30-year-old woman who...
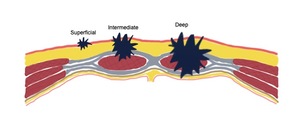
, intermediate (infiltrating the abdominal rectus muscle fascia), and deep (in the abdominal rectus muscle, below fascia).
References: Catarina Mira/ Lisboa 2020")
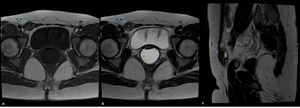
Fig. 8:
Scheme of the abdominal wall showing the classification of abdominal wall...
, T2WI (b) and T1 FSWI (c) showing a hypointense nodule (blue arrow) displaying small hyperintense foci on T1WI consistent with an endometriotic implant.
References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
Fig. 9:
Anterior abdominal wall endometriotic implant in a 29-year-old woman with a...
 and axial T1FS with gadolinium (b) show a heterogeneous nodule on the right abdominal wall infiltrating the rectus abdominis muscle. Axial T2WI (c) after one year of hormonal therapy shows its disappearance.
References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
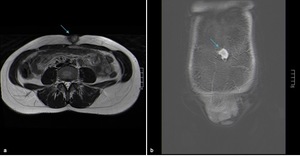
Fig. 10:
Anterior abdominal wall endometriotic implant in a 42-year-old woman with a...
 and coronal T1 FSWI (b) showing a heterogeneous nodule on the umbilicus (blue arrow) displaying the “shading sign” with high signal on T1WI and T1 FSWI and lower signal on T2WI.
References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
Fig. 11:
Umbilical endometriotic implant in a 41-year-old woman. Axial T2WI (a) and...
, axial T2WI (b) and sagittal T2WI (c) showing a hypointense nodule (blue arrow) displaying small hyperintense foci on T1WI consistent with an endometriotic implant. References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
Fig. 12:
Nuck canal implant in a 41-year-old woman. Axial T1WI (a), axial T2WI (b) and...
 and after gadolinium (b) show a hypointense nodule (blue arrow) displaying enhancement after gadolinium. It was surgically removed and pathology confirmed a desmoid tumor (c). References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
Fig. 13:
Anterior abdominal wall lesions infiltrating the left rectus abdominis muscle...
 and coronal T2 WI (b) show umbilical herniation of peritoneal fat.")
Fig. 14:
Umbilical hernia on a 42-year-old woman who felt a lump in the umbilical...

Fig. 15:
Nuck cyst in a 40-year-old woman. Axial T2WI shows a thin-walled cystic lesion...
 with herniation of epiploic fat. References: Department of Radiology, Hospital da Luz de Lisboa/ Lisboa 2019")
Fig. 16:
Inguinal hernia in a 37-year-old woman. Axial T2WI shows right inguinal hernia...

Fig. 17:
Drawing of the female abdominal wall showing the most common locations of...