ECR 2020 / C-13682
Aberrant Origin of the Coronary Arteries: Using Visual and Tactile Aids to Teach Complex Radiologic Concepts
Congress:
ECR 2020
Poster Number:
C-13682
Type:
Educational Exhibit
Keywords:
Cardiac, Anatomy, Cardiovascular system, CT, CT-Angiography, CAD, Congenital, Not applicable
Authors:
P. chiarolanzio1, C. Shilagani2, P. Gerard2, G. Pearson1; 1Valhalla/US, 2Valhalla, NY/US
DOI:
10.26044/ecr2020/C-13682

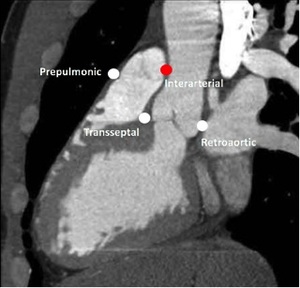
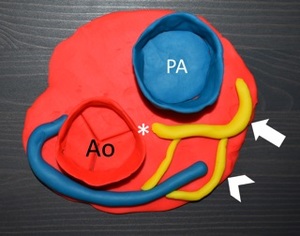
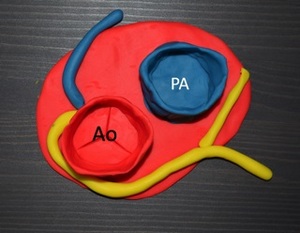
Fig. 1:
Sagittal CT image shows the four potential anomalous locations through the...
. Ao = aorta")
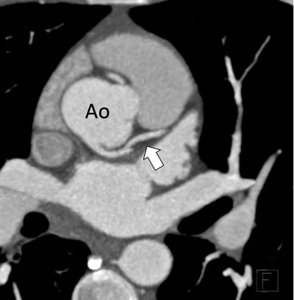
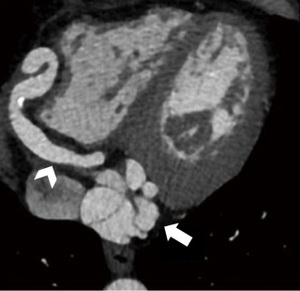
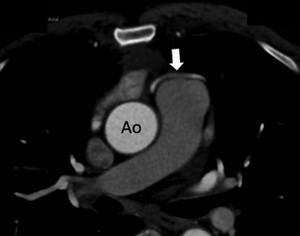
Fig. 2:
White arrow – LMA/Left anterior descending artery (LAD). Ao = aorta

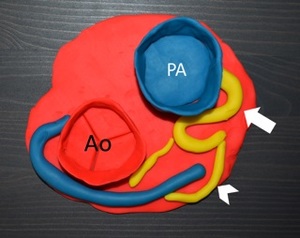
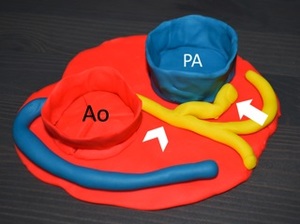
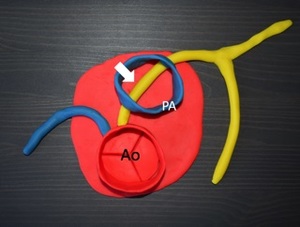
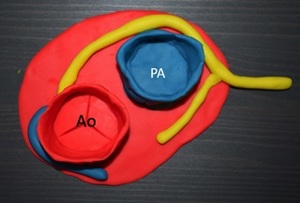
Fig. 3:
Anomalous vessel is in yellow. See the course through the interarterial groove.
 in this pediatric patient. Ao = aorta, PA = pulmonary artery")
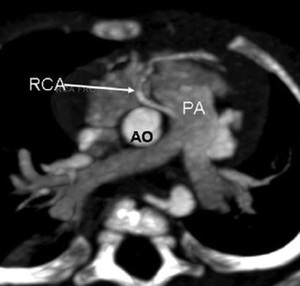
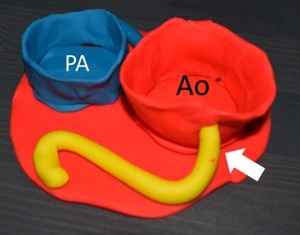
Fig. 4:
White arrow indicates PA origin of the right coronary artery (RCA) in this...

Fig. 5:
Yellow artery demonstrates the PA origin. White arrow = anomalous LMCA. Chevron...
 shows atresia of the LMCA origin, Chevron = smaller yellow collateral arteries filling the main LAD (white arrow).")
Fig. 6:
The asterisk (*) shows atresia of the LMCA origin, Chevron = smaller yellow...
 with the pulmonary artery (white arrow).")
Fig. 7:
Congenital fistula of the LAD (chevron) with the pulmonary artery (white arrow).
 with the LMCA (chevron).")
Fig. 8:
Yellow artery demonstrating the congenital fistula (white arrow) with the LMCA...
.")
Fig. 10:
Clay model with yellow artery demonstrating high origin of the RCA (white...
 arising from the right coronary cusp. Arrow = LAD. B = transseptal course, c= retroaortic course, d = prepulmonic course. References: Prepulmonic Case courtesy of Dr. Yune Kwong, Radiopaedia.org, rID: 29253")
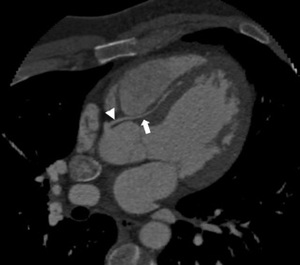
Fig. 11:
CT images of the anomalous LMCA (arrowhead) arising from the right coronary...
 arising from the right coronary cusp. Arrow = LAD. B = transseptal course, c= retroaortic course, d = prepulmonic course. References: Prepulmonic Case courtesy of Dr. Yune Kwong, Radiopaedia.org, rID: 29253")
Fig. 12:
CT images of the anomalous LMCA (arrowhead) arising from the right coronary...
 arising from the right coronary cusp. Arrow = LAD. B = transseptal course, c= retroaortic course, d = prepulmonic course. References: Prepulmonic Case courtesy of Dr. Yune Kwong, Radiopaedia.org, rID: 29253")
Fig. 13:
CT images of the anomalous LMCA (arrowhead) arising from the right coronary...

Fig. 14:
Clay models demonstrating the different courses. Anomalous vessels are...

Fig. 15:
Clay models demonstrating the different courses. Anomalous vessels are...

Fig. 16:
Clay models demonstrating the different courses. Anomalous vessels are...

Fig. 9:
Volumetric rendering showing high origin of the RCA.