ECR 2020 / C-13832
Sonographic "millipede sign": Spontaneous spermatic varicocele thrombosis presenting as acute scrotal pain.
Congress:
ECR 2020
Poster Number:
C-13832
Type:
Educational Exhibit
Keywords:
Not applicable, Varices, Acute, Diagnostic procedure, Ultrasound-Spectral Doppler, Ultrasound-Colour Doppler, Ultrasound, Veins / Vena cava, Vascular, Genital / Reproductive system male, Genitourinary
Authors:
C. Shilagani1, P.-Y. J. sonke2, A. Jednyak3; 1Valhalla, NY/US, 2Tarrytown , ny/US, 3Valhalla/US
DOI:
10.26044/ecr2020/C-13832
.")
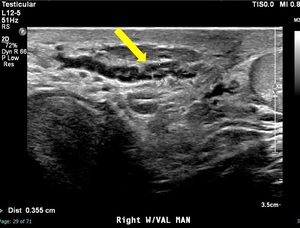
Fig. 1:
There is a curvilinear hypoechoic tubular structure with internal low-level...
.")
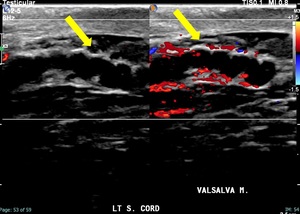
Fig. 2:
Dilated right varicocele does not demonstrate flow on color doppler image...
.")
Fig. 3:
There is a 3.4 mm curvilinear hypoechoic tubular structure in the left...
.")
Fig. 4:
Dilated left spermatic cord vein without internal flow on color doppler image...
.")
Fig. 5:
There is a curvilinear hypoechoic tubular structure with internal low-level...
.")
Fig. 6:
The left spermatic cord vein without internal flow on color doppler image...
.")
Fig. 7:
The left spermatic vein does not demonstrate spectral flow (yellow arrow).