ECR 2020 / C-14261
Hydatid disease : When you dont expect it !
Congress:
ECR 2020
Poster Number:
C-14261
Type:
Educational Exhibit
Keywords:
Abdominal Viscera, Abdomen, Bones, Neuroradiology brain, CT, MR, Ultrasound, Decision analysis, Diagnostic procedure, Localisation, Cysts, Infection, Parasites, Retrospective, Observational, Performed at one institution
Authors:
S. Mghaieth1, B. Khaled2; 1Tunis/TN, 2nabeul/TN
DOI:
10.26044/ecr2020/C-14261

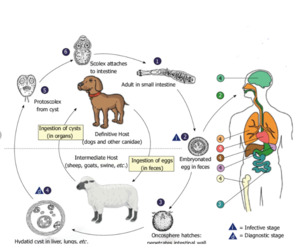
Fig. 2:
Life cycle of Echinococcus granulosus

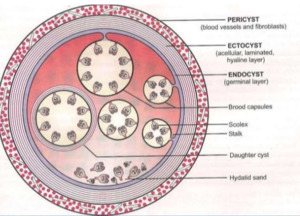
Fig. 3:
The three layers of Hydatid cyst: the pericyst,ectocyst and endocyst.
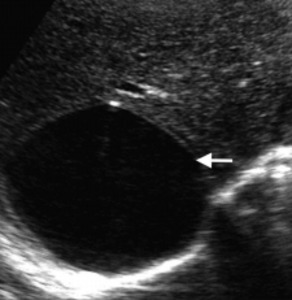
 with posterior acoustic enhancement and a
double-wall sign. References: Mohamed Taher Maamouri Hospital, Nabeul")
Fig. 4:
Type I : liver hydatid cyst. Sonography shows a well-defined
unilocular cyst...
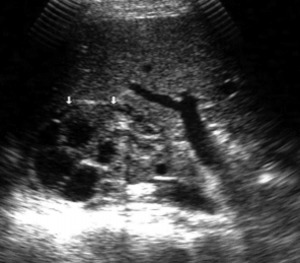
 filling most of the lumen of the mother cyst. References: Mohamed Taher Maamouri Hospital, Nabeul")
Fig. 5:
Sonography shows a lesion with multiple closely placed daughter cysts (arrows)...

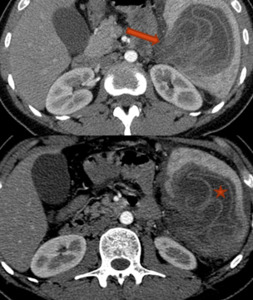
Fig. 6:
Postcontrast axial computed tomography scan shows unilocular cystic lesion

Fig. 7:
Fully calcified mass with serpiginous structures related to a hydatid cyst...

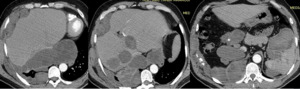
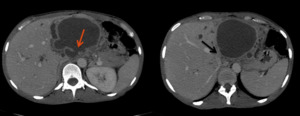
Fig. 8:
Hepatic hydatid cyst ruptured in the peritoneal cavity

Fig. 9:
Splenic hydatid cyst ruptured in the peritoneal cavity

Fig. 10:
Lung hydatid cyst

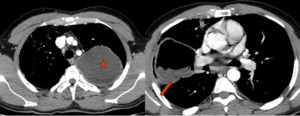
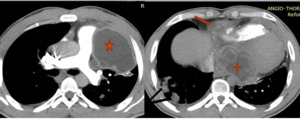
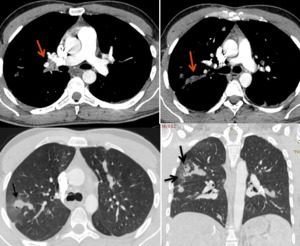
Fig. 11:
Mediastinal window of contrast-enhanced CT images show loculated pericadial...

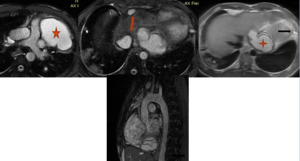
Fig. 12:
Axial T2 weighted MRI images demonstrate high T2 signal, loculated lesions...

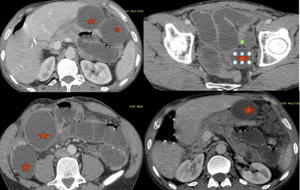
Fig. 13:
SPLENIC, RETROPERITONEAL, HEPATIC AND MEDIASTINAL HYDATIC CYSTS

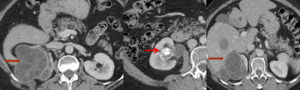
Fig. 14:
Renal hydatid cysts type III and V

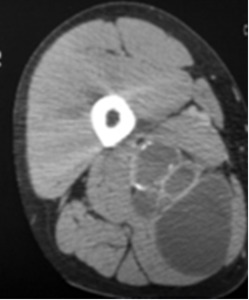
Fig. 15:
Intra-muscular hydatid cyst

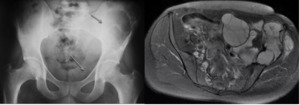
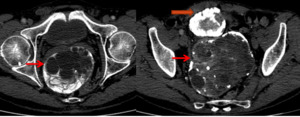
Fig. 16:
HYDATIDOSIS OF THE ILIAC BONE
 References: Mohamed Taher Maamouri Hospital, Nabeul")
Fig. 17:
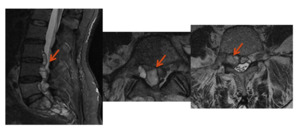
Bone hydatidosis with epidural extension (arrow)

Fig. 18:
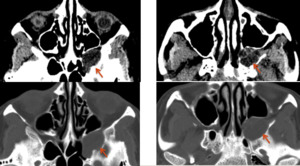
Multilocular cystic formation scalloping on the sphenoidal bone
 with density equal to the LCS ,exerting a mass effect on the median line (arrow) References: Mohamed Taher Maamouri Hospital, Nabeul")
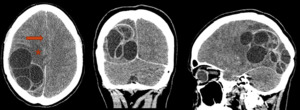
Fig. 19:
Parietal multiloculated intra- axial process surrounded by edema (marked star)...

Fig. 20:
Pelvic hydatid cysts

Fig. 21:
Mechanical occlusion by peritoneal hydatidosis.
, with fluid density. Parenchymal window of contrast-enhanced CT image shows lung hydatid cyst (black arrow). References: Mohamed Taher Maamouri Hospital, Nabeul")
Fig. 22:
Mediastinal window of contrast-enhanced CT image shows occlusion of the right...

Fig. 23:
Open left liver hydatid cysts in the bile ducts with secondary Budd Chiari