ECR 2020 / C-14334
The Paediatric Skull - Fracture or suture
Congress:
ECR 2020
Poster Number:
C-14334
Type:
Educational Exhibit
Keywords:
Education and training, Congenital, Acute, Perception image, Normal variants, Education, CT, Conventional radiography, Trauma, Bones, Anatomy, Paediatric, Not applicable
Authors:
C. Y. Ng, S. H. M. Y. Y. Alqarooni, C. M. Leung, J. H. Fong, J. Foster; Plymouth/UK
DOI:
10.26044/ecr2020/C-14334

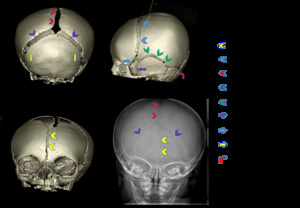
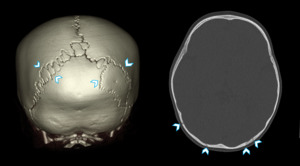
Fig. 1:
3D volume rendered CT images and plain radiograph demonstrating the various...

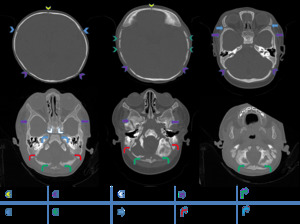
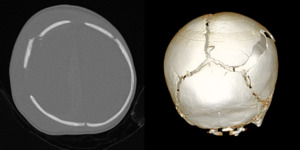
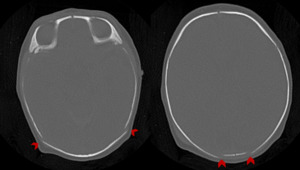
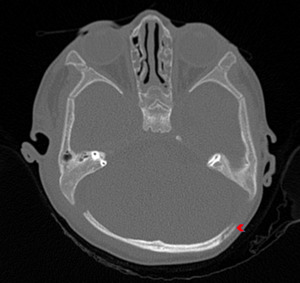
Fig. 2:
Axial CT images of the calvarium and base of skull, demonstrating the cranial...
 and a 3 year old child (Images c & d)
Note the differences in sutural widths of a 6 month old infant and a 3 year old child.")
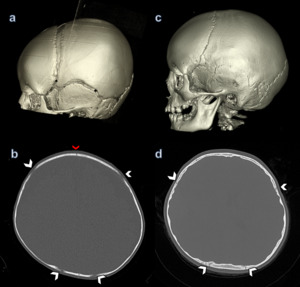
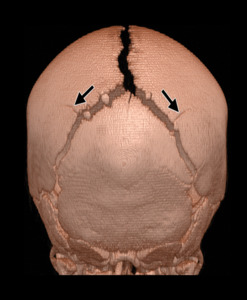
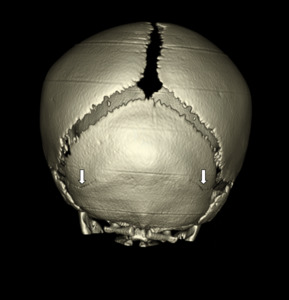
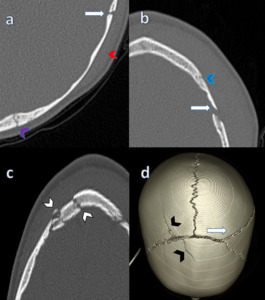
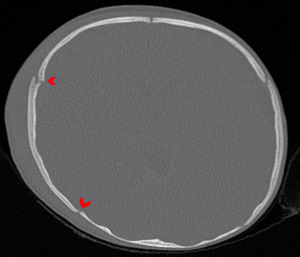
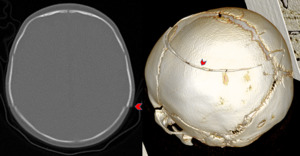
Fig. 3:
3D volume rendered CT and Axial images demonstrating the skull of a 6 month old...
. It is usually obliterated by 7 years of age but can persist to adulthood in 10%. References: S. Idriz, J.H Patel, SA. Renani, R. Allan, I. Vlahos. CT of Normal Developmental and Variant Anatomy of the Paediatric Skull: Distinguishing Trauma from Normality. RadioGraphics RSNA. July 2015; 35(5). DOI : https://doi.org/10.1148/rg.2015140177")
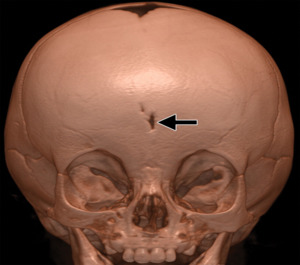
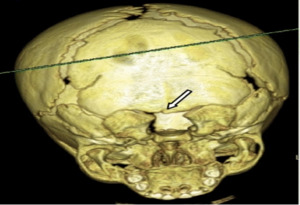
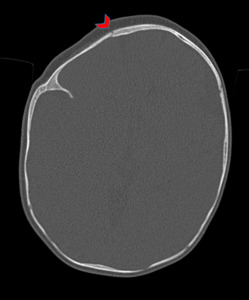
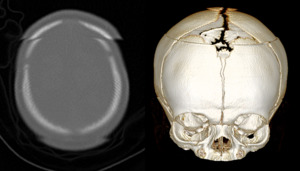
Fig. 4:
3D volume rendered CT image of a persisting metopic suture (Sutura frontalis...
. DOI : https://doi.org/10.1148/rg.2015140177")
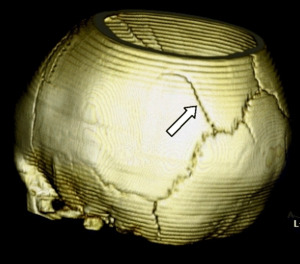
Fig. 5:
3D volume rendered CT image demonstrating bilateral accessory parietal...
: 413-418. DOI: 10.1007/s10140-010-0877-8")
Fig. 6:
3D volume rendered CT image demonstrating a unilateral accessory parietal...
 sutures.")
Fig. 7:
3D volume rendered CT image demonstrating bilateral accessory occipital...
: 413-418. DOI: 10.1007/s10140-010-0877-8")
Fig. 8:
3D volume rendered CT image demonstrating a remnant of the midline occipital...

Fig. 9:
3D volume rendered and axial CT images demonstrating wormian bones. On the...

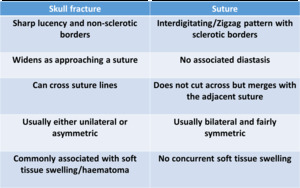
Table 1:
Summary table showing characteristic appearances and differences between...

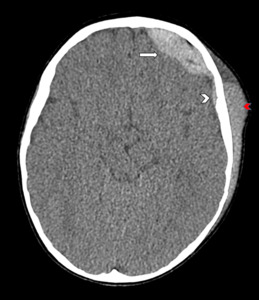
Fig. 10:
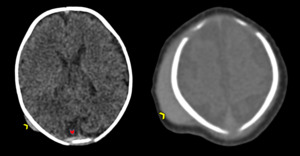
Axial and 3D volume rendered CT images of a 1.5 years old child who sustained a...
 and also a shallow left subdural haematoma (white arrow head). Extracranially, there is a large left subgaleal haematoma (red arrow head).")
Fig. 12:
Axial CT image of the same child, demonstrating a left frontal extradural...

Fig. 13:
Axial CT image of a 2 month old infant.

Fig. 14:
Axial CT image more superiorly demonstrating diastasis of the coronal suture...

Fig. 15:
Axial CT image of a 4 month old infant.
, which can usually also be seen on plain radiographs (aka the Harlequin eye deformity). There is associated asymmetrical growth of the calvarium (white stars).")
Fig. 16:
3D VR demonstrating coronal synostosis in a 4 month old infant and a 3 year old...

Fig. 17:
Axial CT images of a preterm 33/40 weeks neonate.
 and subgaleal haematomas (white arrow heads), associated with a forceps-assisted delivery.")
Fig. 18:
Axial CT images of the same child demonstrating concurrent subdural haematoma...

Fig. 19:
Axial CT image of a 2 month old infant.

Fig. 20:
Axial and 3D volume rendered CT images of a 2 month old infant

Fig. 21:
Further axial and 3D volume rendered CT images demonstrate symmetrical step...