ESCR 2015 / P-0027
The role of myocardial hypoenhancement in patients with non-ST segment elevation acute coronary syndrome
Congress:
ESCR 2015
Poster Number:
P-0027
Type:
Scientific Poster
Keywords:
Cardiac, Cardiovascular system, CT-Angiography, Catheter arteriography, Ultrasound, Contrast agent-intravenous, Arteriosclerosis, Ischaemia / Infarction
Authors:
N. Barysheva, M. Shabanova, D. Ustyuzhanin, T. sukhinina, I. Merculova; Moscow/RU
DOI:
DOI-Link:

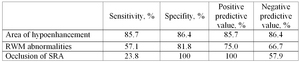
Fig. 1:
The sensitivity, specifity, negative and positive predictive values of the...

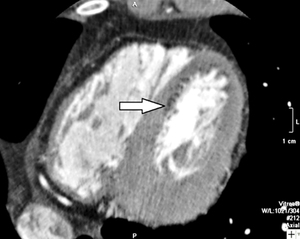
Fig. 2:
Cardiac multidetector computed tomography with contrast enhancement. Myocardial...

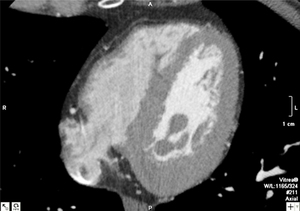
Fig. 3:
Cardiac multidetector computed tomography with contrast enhancement. The same...