Keywords:
Dissection, Contrast agent-intravenous, CT-Angiography, CT, Thorax, Cardiovascular system, Arteries / Aorta
Authors:
E. Muscogiuri1, T. Polidori1, M. Pignatelli2, G. FRAIETTA1, M. Zerunian2, D. Caruso3, D. De Santis4, M. Di Girolamo2, A. Laghi2; 1Roma/IT, 2Rome/IT, 3Rome, lt/IT, 4Roma, Italia/IT
Results
We evaluated 20 patients who underwent various surgery procedures after they were diagnosed with Stanford A AAD.
All the exams were acquired at baseline without ECG triggering. As a consequence, while macroscopic features like the presence of TL and FL or the involvement of other vessels originating from the aorta could be easily detectable, it’s been challenging to clearly assess the presence of an intimal tear. Therefore, we managed to evaluate the presence and thus measure an entry intimal tear only in 5 patients (25%).
The majority of the patients evaluated (12 patients, 60%) were diagnosed with a Stanford A AAD, with an involvement of both thoracic and abdominal aorta (iliac bifurcation involvement). Furthermore, concerning baseline exams, we also evaluated the aortic wall in search of CT signs of atherosclerosis (e.g. plaques, calcifications, etc.): only 6 patients showed no sign of atherosclerosis among the study population. At last, we evaluated the TL and FL: as we expected we found that TL attenuation was 1.29±0.4 times higher than FL. In 6 patients we were also able to assess the presence of thrombi in the false lumen.
We evaluated post-surgery outcome by evaluating residual FL patency and thus evidence of residual or new intimal tears. Only 4 patients (20%) didn’t show a patent FL, while the remaining showed a patent FL but with absent or minimal involvement of ascending aorta and aortic arch (figure 7).
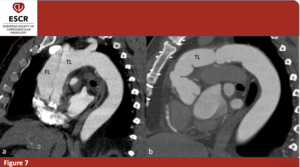
Fig. 7: 63yo M – Pre- and postoperative evaluation of a patient affected by Stanford A AAD. In post-operative CT is not possible to see the FL. (a)(b) sagittal plane only; true (TL) and false (FL) lumina.
As already stated before, the added value of ECG-gated follow-up exam is that this imaging technique allows to better evaluate aorta and aortic valve by removing or at least greatly diminishing motion artifacts. Therefore, we were able to precisely evaluate the presence of distal intimal tears in certain cases of patent FL (figure 8). Furthermore, ECG-gated scans were also useful to evaluate prosthetic aorta integrity and possible misplacement.
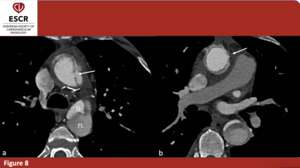
Fig. 8: 57 yo M - ECG-gated CTA of type A aortic dissection (axial plane only) in 57y male patient treated with valve and ascending aorta prosthethic replacement. (a) residual intimal tear (arrow), true (TL) and false (FL) lumina separated by intimal flap in the descending thoracic aorta. (b) Signs of ascending aorta replacement (arrow).

(b) sagittal plane only; true (TL) and false (FL) lumina.")
 in 57y male patient treated with valve and ascending aorta prosthethic replacement. (a) residual intimal tear (arrow), true (TL) and false (FL) lumina separated by intimal flap in the descending thoracic aorta. (b) Signs of ascending aorta replacement (arrow).")