ESSR 2015 / P-0072

Tendon pathologies at the elbow
Congress:
ESSR 2015
Poster Number:
P-0072
Type:
Educational Poster
Keywords:
Trauma, Calcifications / Calculi, Diagnostic procedure, Ultrasound, Plain radiographic studies, MR, Musculoskeletal system, Musculoskeletal soft tissue, Extremities
Authors:
M. Vansevenant1, F. M. H. M. Vanhoenacker2, J. De Roeck3; 1Gent/BE, 2Antwerp, Ghent, Mechelen/BE, 3Herentals/BE
DOI:
10.1594/essr2015/P-0072

Table 1:
Differential diagnosis of lateral epicondylitis

Table 2:
Differential diagnosis of medial epicondylitis

Table 3:
Differential diagnosis of tendon pathology of the posterior compartment

Fig. 7:
Photograph of a patient in “superman”-position with the elbow in extension...
 near the lateral epicondyle suggesting lateral epicondylitis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
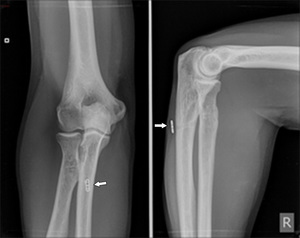
Fig. 8:
Plain film of the elbow showing a soft tissue calcification (arrow) near the...
 in the tendon and a smaller calcification more proximally (curved arrow): calcifying tendinopathy. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
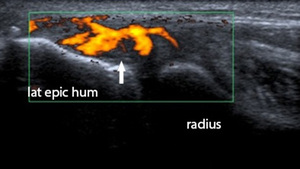
Fig. 9:
Longitudinal ultrasound image of the common extensor tendon showing a large...
 in the tendon: hyperemia. This hyperemia is caused by an angiofibroblastic reaction, the repairative response to the (micro-)tearing with the formation of scar tissue. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
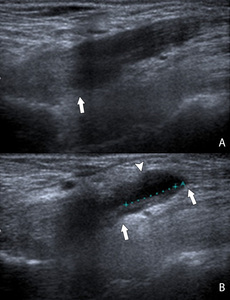
Fig. 10:
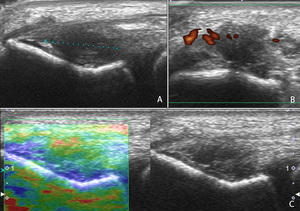
Longitudinal ultrasound image of the common extensor tendon showing increased...
 and transversal (B) ultrasound image of the extensor tendons showing a hypoechogenic zone (A,B,C) within the extensor tendons: tendinosis. There is an increased Doppler signal (B): hyperemia. The zone of tendinosis has on elastography (C) an increased compressibility of the tendon. The blue spots on the color map represent hard tissue with low compressibility and the red spots represent soft tissue with high compressibility. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 11:
Longitudinal (A,C) and transversal (B) ultrasound image of the extensor tendons...
 T2-WI of the normal elbow. A is 2 slices anterior of B. The common extensor tendon (arrow) inserts on the lateral epicondyle and is in normal circumstances hypointense on all imaging sequences. The radial collateral ligament is deep of the common extensor tendon situated (curved arrow). The lateral ulnar collateral ligament is located posteriorly to the radial head. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 12:
Coronal fat saturated (FS) T2-WI of the normal elbow. A is 2 slices anterior of...
: partial tear. There are no associated lesions. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
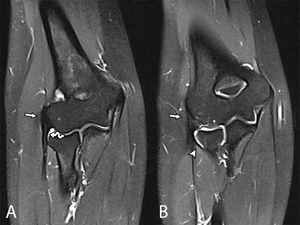
Fig. 13:
Coronal T2-WI with FS showing a thickened common extensor tendon with a...
 T2-WI with FS and axial (B) dixon T2-WI with FS showing a severe tear of the conjoint extensor tendon (arrow) with perilesional edema (arrowhead). There is an associated radial collateral ligament rupture at its insertion on the lateral epicondyle, resulting in posterolateral rotatory instability of the elbow (curved arrow). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
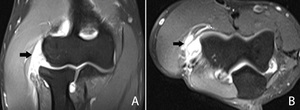
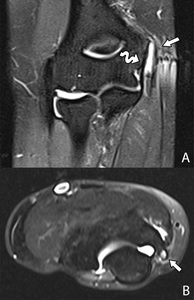
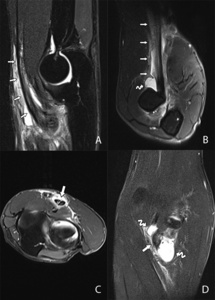
Fig. 14:
Coronal (A) T2-WI with FS and axial (B) dixon T2-WI with FS showing a severe...
 and axial (B) T2-WI with FS showing a full thickness tear of the conjoint tendon with retraction and involvement of the radial collateral ligament. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 15:
Coronal (A) and axial (B) T2-WI with FS showing a full thickness tear of the...

Fig. 16:
Coronal pd T2-WI with FS showing a post-traumatic tear of the insertion of the...
 and a sagittal T1-WI of a patient with Panner's disease (B). In Panner's disease, there is also involvement of the growth plate and it is seen in children between the age of 7-12 years old. Osteochondritis dissecans is usually seen in young adolescents between the age of 12-15 years old. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 17:
Sagittal T2-WI with FS of a patient with an osteochondritis dissecans (A) and a...

Fig. 18:
Axial T2-WI with FS of a patient with a radial tunnel syndrome showing edema in...
 near the medial epicondyle suggesting medial epicondylitis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
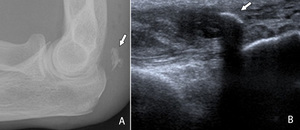
Fig. 19:
Plain film of the elbow showing a soft tissue calcification (arrow) near the...
 and transversal (B) plane of the flexor-pronator mass showing a calcification surrounded by hypoechogenicity: medial epicondylitis. Both planes are necessary to be able to exactly locate the lesion in the anterior aspect of the tendon. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
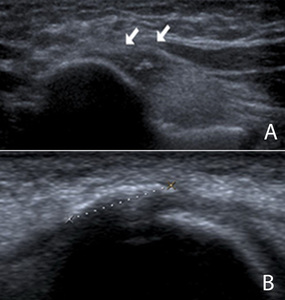
Fig. 20:
Ultrasound in a longitudinal (A) and transversal (B) plane of the...
 inserts on the medial epicondyle and is in normal circumstances hypointense on all imaging sequences. The medial collateral ligament is deep of the flexor-pronator mass situated (curved arrow). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 21:
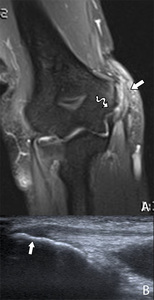
Coronal T2-WI with FS of the normal elbow. The flexor-pronator mass (arrow)...
 with in the same patient a corresponding ultrasound image in the longitudinal plane at the flexor-pronator mass (B). The MRI shows thickening and hyperintensity (arrow) at the tendon of the flexor-pronator mass. Adjacent bone marrow edema is seen in the medial epicondyle. There is also a rupture of the medial collateral ligament at the insertion on the medial epicondyle (curved arrow). The ultrasound image shows the same tendon thickening with accompanying hypoechogenicity: medial epicondylitis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 22:
Coronal pd T2-WI with FS (A) with in the same patient a corresponding...
 and axial (B) pd T2-WI with FS showing a hypointense zone in the tendon of the flexor-pronator mass. Some fibers are still attached to the medial epicondyle (arrow): partial tear. The MCL has a normal insertion on the medial epicondyle (curved arrow). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 23:
Coronal (A) and axial (B) pd T2-WI with FS showing a hypointense zone in the...
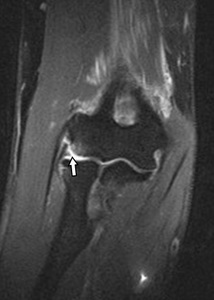
, axial (B) and sagittal (C) T2-WI showing a complete tear of the flexor-pronator mass (arrow). The degree of retraction should be evaluated on sagittal images (distance between the curved arrows). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
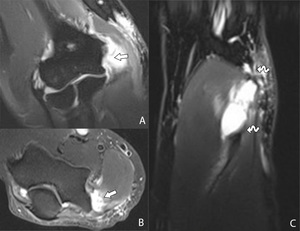
Fig. 24:
Coronal (A), axial (B) and sagittal (C) T2-WI showing a complete tear of the...
 show the avulsion fragment (arrow) and a traumatic separation of the medial epicondyle apophysis (curved arrow) with accompanying soft tissue swelling. A subsequent MRI of the elbow reveals an avulsion fragment (arrow) on the pd T2-WI with FS (B). The tendons of the flexor-pronator mass do not seem to be ruptured (arrowhead). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 25:
Avulsion fracture of the medial epicondyle after a valgus trauma in a...
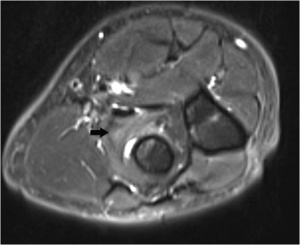
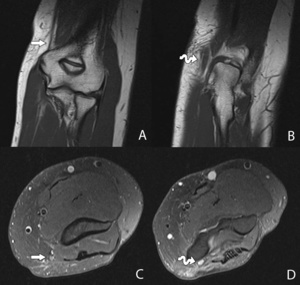
 and more proximally (A). Corresponding T2-WI in the axial plane at the level of the cubital tunnel (D) and more proximally (C). The ulnar nerve in the cubital fossa is thickened and hyperintense on the T2-WI compared to the images more proximally: ulnar neuropathy. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 26:
Coronal T1-WI of the elbow showing the ulnar nerve in the cubital tunnel (B)...
 after repair of the MCL and the flexor-pronator mass. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 27:
Plain film of the elbow showing a Mitek-anchor (arrow) after repair of the MCL...
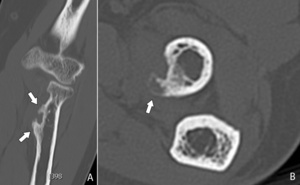
 and axial (B) CT-image in bone window of the elbow revealing a bone spur formation at the radial tuberosity (arrows). This can be misinterpreted as a tumor. The key to the diagnosis is the location at the insertion of the biceps tendon and the absence of a soft tissue mass. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 28:
Coronal (A) and axial (B) CT-image in bone window of the elbow revealing a bone...
 and a soft tissue collection is seen (arrowhead). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 29:
Longitudinal ultrasound image of the distal biceps tendon revealing a partial...

Fig. 30:
The FABS position is used to obtain a straight distal biceps tendon in a...
, axial (C) and coronal (D) T2-WI with FS and T2-WI with FS in FABS position (B). The distal tendon of the biceps muscle is hyperintense (arrows) on the sagittal image and on the image in FABS position with fluid signal intensity around the tendon (arrows): tendinosis of the distal biceps tendon with peritendinosis. Notice the better visualization of the distal portion of the biceps tendon in FABS position compared to the standard position in extension. On the axial images, a hyperintense longitudinal cleft (arrow) can be seen: partial longitudinal tear. Along the biceps tendon, a hyperintense, sharply delineated structure is seen (curved arrows): bicipitoradial bursitis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 31:
Sagittal (A), axial (C) and coronal (D) T2-WI with FS and T2-WI with FS in FABS...
 and an axial T1-WI at the level of the lacertus fibrosis (B). There is a full thickness tear at the radial tuberosity seen with retraction of 3,5 cm. The lacertus fibrosis is still intact (arrow), causing the biceps tendon not to retract any further. Retraction of more than 8 cm indicates rupture of the lacertus fibrosis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 32:
Dixon T2-WI with FS in FABS position at the level of the radial tuberosity (A)...
 after distal biceps tendon repair. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 33:
Plain films of the elbow showing anchor placement (arrow) after distal biceps...
 at the olecranon. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 34:
Plain films showing spur formation (arrow) at the olecranon.
: calcifying tendinosis of the distal triceps tendon. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 35:
Ultrasound of the distal triceps tendon showing thickening of the tendon,...
 and axial (B) T2-WI with FS showing hyperintensity at the distal portion of the triceps tendon (arrow) and peritendinous hyperintensity: tendinosis of the distal triceps tendon with peritendinosis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 36:
Sagittal (A) and axial (B) T2-WI with FS showing hyperintensity at the distal...
 of the elbow and ultrasound (B) of the distal triceps tendon showing an avulsion fragment of the olecranon (arrow). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 37:
Plain films (A) of the elbow and ultrasound (B) of the distal triceps tendon...
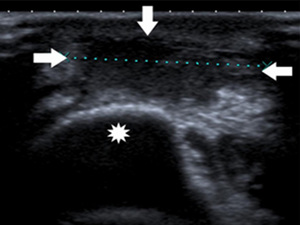
 in the subcutaneous soft tissue at the olecranon (star): olecranon bursitis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
Fig. 38:
Ultrasound of the posterior elbow showing a fluid collection (arrows) in the...