Elbow tendinosis is very frequent in daily practice and is often attributed to overuse or intensive sports activities.
Microtearing occurs during stress on a tendon.
If the stress is repetitive,
there will be no fully repair because of the hypovascular nature of a tendon and the repetitiveness of the stress with new microtearing.
This results in tendinosis and eventually macrotears.
As a reaction to the (micro)tearing of the tendon,
an angiofibroblastic reaction occurs with the formation of scar tissue,
being very vulnerable to repetitive trauma resulting in new and further tearing.
Direct trauma is another cause of tendon injury and the mechanism of trauma differs along with the involved compartment.
The therapeutical strategy depends on the involved compartment and the mechanism of injury.
Clinical examination and history is a prerequisite for correct diagnosis.
In most scenarios,
there is no need for additional imaging.
In therapy resistant or severe cases or in the presence of confounding symptoms,
imaging becomes mandatory.
Serious tendon pathology or associated abnormalities must not be overlooked.
Imaging is also useful to aid in the preoperative planning.
The elbow joint can be divided in 4 compartments: the lateral,
medial,
anterior and posterior compartment.
Each compartment is reviewed to its anatomy and tendon pathology with their respective differential diagnosis.
A) The lateral compartment
The lateral compartment is the most affected compartment of the elbow.
The extensor muscles of the elbow attach at the lateral epicondyle: the extensor carpi radialis longus,
extensor carpi radialis brevis,
extensor digitorum communis and extensor carpi ulnaris tendon (from ventral to dorsal).
The last three tendons form the strong common extensor tendon,
attached to the anterior aspect of the lateral epicondyle ( Fig. 1 ).
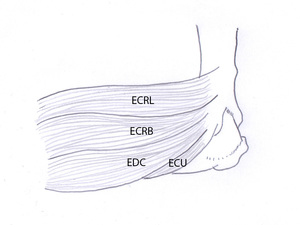
Fig. 1: Drawing of a lateral view of the elbow showing the insertion of the common extensor tendon (the extensor carpi radialis brevis (ECRB), the extensor digitorum communis (EDC) and the extensor carpi ulnaris (ECU)) and the extensor carpi radialis longus tendon (ECRL). The extensor carpi radialis brevis tendon is most frequently injured in lateral epicondylitis. The second most affected tendon is the extensor digitorum communis tendon.
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
The lateral collateral ligament consists of the lateral ulnar collateral ligament,
accessory lateral collateral ligament (inconsistently present),
annular ligament and radial collateral ligament ( Fig. 2 ).
All of them are attached to the lateral epicondyle except the annular ligament being attached to the anterior and posterior radial notch on the ulna.
The annular ligament encircles the proximal radius to hold it against the ulna.
The radial collateral ligament joins anteriorly with the fibers of the annular ligament and joins with the fascia of the supinator muscle.
The lateral ulnar collateral ligament inserts on the supinator crest of the ulna and gives primarily resistance to varus stress.
There is no attachment of the lateral collateral ligament to the radius to allow pronation and supination.
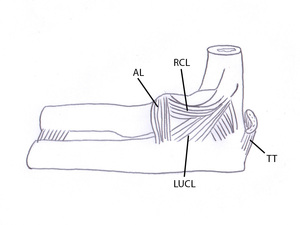
Fig. 2: Drawing of a lateral view of the elbow showing the lateral collateral ligament: the annular ligament (AL), the lateral ulnar collateral ligament (LUCL) and the radial collateral ligament (RCL). The distal triceps tendon is attached at the posterior side of the olecranon.
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
Lateral epicondylitis or tendinosis is caused by repetitive contraction of the extensor muscles.
The extensor carpi radialis brevis is most frequently injured in lateral epicondylitis.
The undersurface of this tendon slides over the capitellum during flexion and extension of the elbow.
The second most affected tendon in lateral epicondylitis is the extensor digitorum communis tendon.
In severe cases of lateral epicondylitis or post-traumatic,
the lateral ulnar collateral ligament and radial collateral ligament can be injured.
The clinical features of lateral epicondylitis are lateral elbow pain,
provoked by wrist extension and with grasping of objects.
Occupations requiring wrench movements are very prone to lateral epicondylitis.
It is also seen in racket sporters with backhand swings.
Palpation of the tendon insertion at the lateral epicondyle is painful.
History and clinical examination is usually sufficient to make the right diagnosis.
In most scenario’s,
imaging is not required.
Lateral epicondylitis is sometimes accompanied by a lesion of the lateral collateral ligament,
resulting in a posterolateral rotatory instability during varus stress.
There are various other (less frequent) differential diagnoses of pain at the lateral compartment of the elbow ( Table 1 ).
Another cause of tear of the extensor tendons and/or lateral collateral ligament is trauma.
The mechanism of trauma is varus stress on the elbow.
In children,
avulsion of the epicondyle is more frequent than tear of the tendons.
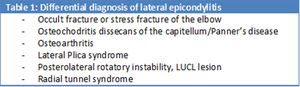
Table 1: Differential diagnosis of lateral epicondylitis
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
A radial tunnel syndrome has been reported in up to 5% of the patients with an initial clinical diagnosis of epicondylitis lateralis.
It is caused by an entrapment of the posterior interosseus nerve in the radial tunnel.
It is associated with repetitive pronation and supination.
Osteochondritis dissecans (osteochondral lesion) is a possible differential diagnosis of lateral elbow pain,
typically seen in throwing sporters between the ages of 12-15 years old.
It is caused by repetitive stress at the lateral elbow resulting in a lesion of the cartilage and subchondral bone.
In Panner's disease on the other hand,
the growth plate is also affected.
Panner's disease is seen at a younger age (7-12 years old).
The treatment of lateral epicondylitis is primarily conservative with relative rest,
immobilization,
ice application and nonsteroidal anti-inflammatory drugs (NSAID) or corticosteroid injections.
If conservative treatment fails after 3-6 months,
surgery can be performed with release and debridement of the degenerated tendon.
B) The medial compartment
The medial compartment is the second most affected compartment.
The medial epicondyle serves as attachment of the flexor muscles of the elbow.
The flexor-pronator mass (pronator teres and flexor carpi radialis) is most frequently injured.
The other flexor tendons are the palmaris longus,
flexor carpi ulnaris,
flexor digitorum and flexor digitorum superficialis.
The attachment of the flexor-pronator mass and the flexor carpi ulnaris is at the anterior aspect of the medial condyle ( Fig. 3 ).
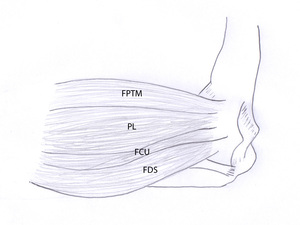
Fig. 3: Drawing of a medial view of the elbow showing the insertion of the flexor-pronator teres mass (FPTM) (pronator teres and flexor carpi radialis tendon), palmaris longus (PL), flexor carpi ulnaris (FCU) and flexor digitorum superficialis. The flexor-pronator mass is most frequently injured in lateral epicondylitis.
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
The medial collateral ligament (ulnar collateral ligament) is composed of three bundles (an anterior,
posterior and oblique band),
forming a triangular shaped ligament with the apex oriented to the medial epicondyle.
The base is oriented on the ulna.
The anterior band gives the most constraint to valgus stress.
The posterior and oblique band forms the floor of the cubital tunnel,
containing the ulnar nerve ( Fig. 4 ).
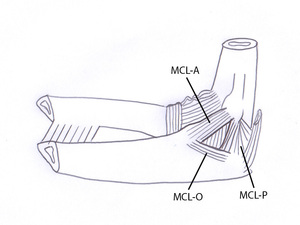
Fig. 4: Drawing of a medial view of the elbow showing the medial collateral ligament. It is composed of an anterior (MCL-A), posterior (MCL-P) and an oblique bundle (MCL-O). The posterior and oblique bundle form the floor of the cubital tunnel containing the ulnar nerve.
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
Medial epicondylitis is caused by repetitive contraction of the flexor muscles of the elbow and valgus stress.
This is typically seen in golfers and in sports with overhand throwing.
The flexor-pronator mass is most prone to injury,
followed by the palmaris longus.
In severe cases,
the medial collateral ligament and ulnar nerve can also be injured.
The clinical features of medial epicondylitis are medial elbow pain,
provoked by flexion of the wrist.
Golfers,
overhead throwing sporters and racket sporters with forehand stroke are very prone to medial epicondylitis.
Symptoms of ulnar neuritis can also be present in patients with associated injury to the ulnar nerve.
Palpation of the tendons at the medial epicondyle is very painful.
As in lateral epicondylitis,
clinical examination with history is usually sufficient to make the right diagnosis.
As in lateral epicondylitis,
medial epicondylitis can be accompanied by a lesion of the ulnar collateral ligament.
Trauma will rather cause avulsion of the medial epicondyle than tear of the flexor tendons.
The mechanism is a trauma with valgus stress on the elbow.
There are various other (less frequent) differential diagnoses of pain at the medial compartment of the elbow ( Table 2 ).
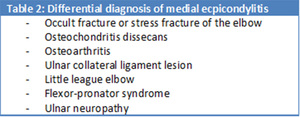
Table 2: Differential diagnosis of medial epicondylitis
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
The ulnar nerve is frequently injured (cubital tunnel syndrome) in medial epicondylitis and should always be evaluated in patients suspected with medial epicondylitis.
The flexor-pronator syndrome is an entrapment syndrome of the median nerve at its course between the two heads of the pronator teres muscle.
It is much less frequent than the radial tunnel syndrome.
A little league elbow is an avulsion of the medial epiphyseal growth plate caused by repetetive valgus stress on the elbow.
It is seen in baseball pitchers under the age of 16 years old.
Treatment of medial epicondylitis is primarily conservative consisting of relative rest,
immobilization,
ice application and nonsteroidal anti-inflammatory drugs (NSAID) or corticosteroid injections.
If conservative treatment fails after 3-6 months,
surgery can be performed with release and debridement of the degenerated tendon.
Surgery is sometimes performed earlier in professional sportsmen.
C) The anterior compartment
The tendon pathology of the anterior compartment is limited to the distal biceps brachii tendon.
The distal biceps tendon is inserted at the ulnar tuberosity ( Fig. 5 ,
Fig. 6 ).
As a supinator of the forearm,
the tendon is turned around the ulnar aspect of the proximal radius in pronation.
The tendon unwinds during contraction of the biceps muscle with supination of the forearm as a result ( Fig. 6 ).
The lacertus fibrosis (bicipital aponeurosis) also arises from the distal musculotendinous junction of the biceps,
inserting eventually onto the proximal ulna after enforcing the fascia of the ventral forearm ( Fig. 5 ).
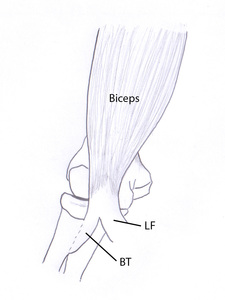
Fig. 5: Drawing of an anterior view of the elbow. The distal biceps brachii muscle tendon (BT) inserts on the radial tuberosity, situated more posteriorly in pronation than in supination. The lacertus fibrosis (LF) or bicipital aponeurosis inserts on the fascia of the forearm and the ventral aspect of the ulna.
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
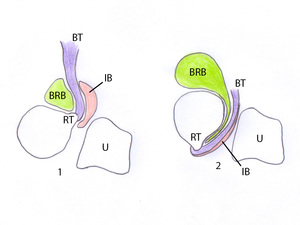
Fig. 6: Drawing of a transversal plane of the radius and ulna showing the distal biceps tendon (BT) being wound around the radius in pronation (2) and rotating the radius by pulling the radial tuberosity to a ventral position to acquire supination (1). A bicipitoradial bursa (BRB) and an interosseous bursa (IB) facilitate the movement between the radius, biceps tendon and ulna (U).
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
A full thickness tear of the biceps tendon with rupture of the lacertus fibrosis is in most cases clinically clear without imaging.
There is a history of a severe trauma with a large force against a flexed elbow.
A sudden “snap” can be felt sometimes,
associated with sudden severe pain.
Complete tears without rupture of the lacertus fibrosis and partial tears of the distal biceps tendon are less clear clinically.
Partial tears are associated with a minor trauma or even no trauma at all,
suggesting a preexisting tendinosis.
Most tears occur at about 1 to 2 cm from the insertion on the radial tuberosity because of a relative hypovascularity in this region.
Mechanical impingement is a risk factor for tearing of the distal biceps tendon.
This impingement can be caused by osteophytes and enthesophytes near the radial tuberosity or by pronation.
The bicipitoradial or interosseous bursa around the distal biceps tendon ( Fig. 6 ) can get irritated resulting in cubital bursitis.
A lump can be felt in the cubital fossa.
Secondary compression syndromes of the median or posterior interosseous nerves occurs in rare cases.
The most frequent cause of bursitis in this region is repeated mechanical trauma and is often associated to partial tearing of the distal biceps tendon.
Treatment of a complete tear of the distal biceps tendon is early surgical repair.
Partial tears are most frequently treated by relative rest,
immobilization,
ice application and nonsteroidal anti-inflammatory drugs (NSAID) or corticosteroid injections.
At failure of conservative treatment,
surgical debridement of remaining fibers with tendon reattachment can be necessary.
D) The posterior compartment
The posterior tendon compartment is only rarely injured and is limited to pathology of the distal triceps brachii tendon.
The distal triceps tendon attaches at the posterior aspect of the olecranon ( Fig. 2 ).
There is also an extension to the forearm situated superficially of the anconeus muscle.
As in the other compartments,
repetitive stress on the distal triceps tendon causes tendinosis.
It is seen in sporters performing a lot of pushing activities (e.g.
pushups,
dips or boxing).
Clinical examination reveals pain during stretching of the triceps muscle and palpatory pain at the distal insertion of the triceps tendon.
Tearing of the distal triceps tendon can be partial or complete.
A possible mechanism of rupture is a fall on an outstretched hand.
Olecranon bursitis is the most frequent differential diagnosis of tendon pathology of the posterior compartment.
Other differential diagnoses are less frequent ( Table 3 ).

Table 3: Differential diagnosis of tendon pathology of the posterior compartment
References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium
A frequent cause of pain at the posterior elbow is an olecranon bursitis.
It is associated with a soft tissue swelling.
Posterolateral rotatory instability is also a differential diagnosis in the posterior compartment,
just as in the lateral compartment.
Valgus extension overload syndrome is caused by osteophytes,
loose bodies or chondromalacia at the olecranon and posteromedial fossa.
It is typically seen in baseball pitchers.
A cubital tunnel syndrome is frequently associated with this condition.
The same treatment options as in the other compartments are available for the posterior compartment.
The threshold to proceed to surgical repair of a tear is lower as in the anterior compartment because the triceps muscle is an important muscle for extension of the elbow whereas in the anterior compartment,
flexion can be partially taken over by the brachialis muscle.


, the extensor digitorum communis (EDC) and the extensor carpi ulnaris (ECU)) and the extensor carpi radialis longus tendon (ECRL). The extensor carpi radialis brevis tendon is most frequently injured in lateral epicondylitis. The second most affected tendon is the extensor digitorum communis tendon. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
, the lateral ulnar collateral ligament (LUCL) and the radial collateral ligament (RCL). The distal triceps tendon is attached at the posterior side of the olecranon. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")

 (pronator teres and flexor carpi radialis tendon), palmaris longus (PL), flexor carpi ulnaris (FCU) and flexor digitorum superficialis. The flexor-pronator mass is most frequently injured in lateral epicondylitis. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
, posterior (MCL-P) and an oblique bundle (MCL-O). The posterior and oblique bundle form the floor of the cubital tunnel containing the ulnar nerve. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")

 inserts on the radial tuberosity, situated more posteriorly in pronation than in supination. The lacertus fibrosis (LF) or bicipital aponeurosis inserts on the fascia of the forearm and the ventral aspect of the ulna. References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
 being wound around the radius in pronation (2) and rotating the radius by pulling the radial tuberosity to a ventral position to acquire supination (1). A bicipitoradial bursa (BRB) and an interosseous bursa (IB) facilitate the movement between the radius, biceps tendon and ulna (U). References: Department of Radiology, AZ Sint-Maarten, Mechelen-Duffel, Belgium")
