♦ Introduction
PHP involves a heterogeneous group of disorders caused by target-organ resistance to the action of parathyroid hormone (PTH),
manifesting with diverse clinical and radiographic features.
♦ Epidemiology
◊ Prevalence: Extremely rare disorder [Japan study,
1997:
3.4 (2.6-4.2) cases per 1 million people]
◊ Gender ratio: Women/Men : 2/1
◊ Most common subtype: Ia / Rarest subtype: Ic
◊ Time of onset: Variable (from toddlerhood until late adulthood)
♦ Pathogenesis - Classification
◊ Variants:
Four PHP variants have been described: Type Ia,
Ib,
Ic and II.
PHP Ia is primarily characterized by variable signs of delayed skeletal growth,
usually presenting with physical features of Albright hereditary osteodystrophy (AHO).
This skeletal phenotype is rarely present in a proportion of patients with PHP Ic.
PHP I: Associated with reduced urinary cAMP and phosphate excretion.
- Subtype Ia: Resistance to PTH and other hormones that stimulate adenyl cyclase in their target tissues,
such as TSH.
Autosomal dominant pattern of inheritance,
attributed to haploinsufficiency of GNAS1.
- Subtype Ib: Mainly renal resistance to PTH.
Considered as sporadic,
although familial cases have been reported.
Inherited as an autosomal dominant trait,
but mutations in the PTH gene or PTH receptor genes have not been determined.
Investigators (Jüppner et al,
1998) have mapped the gene to a small region of band 20q13.3,
very near the GNAS1 gene .There is also a hypothesis on a mutation in the carboxyl terminus of the GNAS1 gene (Wu et al,
2001).
- Subtype Ic: Resistance to PTH and other hormones in defiance of non-established Gs abnormal activity.
Mutations in the C-terminal of the GNAS gene have been mapped,
though.
Note that PHP-Ia and Ic patients share multihormone resistance (to PTH,
TSH and FSH/LH) as well as the Albright Hereditary Osteodystrophy (AHO) phenotype.
PHP II: Characterized by normal urinary cAMP excretion and reduced phosphate excretion.
Patients lack the somatic anomalies associated with AHO.
The inheritance mode is yet to be designated,
but there is a hypothesis on an acquired defect secondary to vitamin D deficiency.
» Pseudopseudohypoparathyroidism (PPHP) is a condition genetically related to PHP-Ia,
sharing the same signs and symptoms,
but showing no resistance to PTH as seen in individuals with PHP-Ia.
Both PHP-Ia and PPHP are caused by mutations that affect the function of the GNAS gene.
◊ Genetics:
Mutations affecting the Gs(alpha) protein-encoding GNAS exons (guanine nucleotide binding protein,
alpha stimulating - complex locus),
have been identified as the underlying etiological factor.
The PTH receptor is coupled to the stimulatory G protein (Gs),
mediating the cAMP signal transduction pathway.
Therefore,
measuring serum and urinary cAMP levels following administration of bovine PTH,
permitts the differentiation between PHP type I,
related to blunted cAMP response to PTH and PHP type II in which the cAMP response is conserved.

Fig. 1: Graphical network of the top 20 diseases related to Pseudohypoparathyroidism.
References: Weizmann Institute of Science - www.malacards.org
♦ Clinical presentation
- AHO phenotype: Short stature,
rounded face,
developmental delay and mental retardation (usually mild),
centripetal obesity,
shortening of metacarpal and metatarsal bones (charasterically 4rth and 5th),
dental hypoplasia,
soft-tissue ossification.
- Signs of hypocalcemia: Carpopedal muscular spasms,
cramping,
numbness and tetany,
as well as generalized seizures,
when the calcium deficit is severe.
Paraesthesias affecting the lips,
fingers or toes are common early symptoms.
Hyperphosphatemia can induce an increase in the deposition of calcium phosphate in extraskeletal tissues,
causing nephrolithiasis,
cataracts and subcutaneous calcifications.
- Hormone deficiency symptoms (TSH,
ADH,
ACTH,
GH,
FSH/LH,
Glucagon)
- Reproductive system disorders/Hypogonadism: ◊ Females: Delayed puberty,
oligomenorrhea,
infertility ◊ Males: Testicular descent disorders,
infertility
- Skeletal anomalies: Brachydactyly,
shortened ulna,
radial and tibial bowing,
angular elbow dysplasia,
coxa vara/valga,
tibia vara/valga.
- Atypical clinical manifestations: Neonatal hypothyroidism,
Parkinson disease,
spinal cord compression.
Subjects with types Ia and Ic usually demonstrate the characteristic skeletal phenotype of AHO.
PHP-Ia is most typically manifested by bone resorption with blunting and shortening of the fourth and fifth metacarpal bones,
most notable when the dorsum of the hand is viewed in closed-fist position (Archibald's sign).
» Patients with PHP may be asymptomatic,
mainly in childhood and adolescence.
♦ Laboratory studies
The biochemical profile of PHP patients includes elevated serum concentrations of PTH and phosphate with low or normal serum levels of ionized calcium.
In addition to PTH resistance,
almost all PHP-Ia patients present with resistance to TSH,
with usually faintly elevated TSH levels and normal or slightly decreased thyroid hormone levels.
Prolactin and GH deficiency has been documented in some PHP-Ia subjects,
while resistance to calcitonin has also been occasionally described.
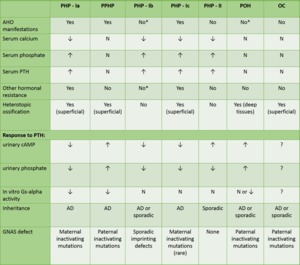
Fig. 2: Clinical, Biochemical, and Genetic Features of Pseudohypoparathyroidism and Related Disorders:
*Except for some cases.
PHP: pseudohypoparathyroidism; PPHP: pseudopseudohypoparathyroidism; POH: progressive osseous heteroplasia; OC: osteoma cutis; AHO: Albright's hereditary osteodystrophy; PTH: parathyroid hormone; cAMP: cyclic adenosine monophosphate; GNAS: guanine nucleotide-binding protein, alpha-stimulating activity polypeptide; Downwards arrow: decreased; Upwards arrow: increased; N: normal; AD: autosomal dominant.
References: Manuel C. Lemos and Rajesh V. Thakker (2014),
♦ Imaging findings
- Plain radiography: The main imaging procedure,
sufficiently depicting PHP skeletal changes.
◊ Shortening of metacarpals and metatarsals (symmetric or
asymmetric): Descending order of frequence: 4rth,
5th,
3rd,
1st,
2nd
◊ Shortening or deformation of phalanges (most frequently the
distal and medial)
◊ Metaphyseal resorption
◊ Epiphyseal anomalies: Premature epiphyseal fusion of the tubular
bones,
cone-shaped epiphyses of digits
◊ Widened trabeculae
◊ Diffuse osteopenia
◊ Osteosclerosis
◊ Soft-tissue calcification/ossification: skin,
subcutaneous tissue,
deep
connective tissue
◊ Exostoses
◊ Bowed radius and ulna
◊ Coxa vara/coxa valga
◊ Calvarial thickening
◊ Abnormal dentition: hypoplasia,
defective dentine,
widened root
canals,
delayed eruption,
excessive caries.
- CT/MRI: Imaging techniques used to demonstrate probable CNS and ocular manifestations of the disease.
◊ Basal ganglia calcification
◊ Deep white matter calcification
◊ Sclerochoroidal calcification
