ESSR 2016 / P-0013
Lesions of the Mandible in Children: A Pictorial Approach to Differential Diagnosis
Congress:
ESSR 2016
Poster Number:
P-0013
Type:
Educational Poster
Keywords:
Education and training, Cysts, Cancer, Education, Computer Applications-Detection, diagnosis, Computer Applications-3D, Ultrasound, MR, CT, Paediatric, Musculoskeletal bone, Musculoskeletal system
Authors:
E.-L. H. J. Teo; Singapore/SG
DOI:
10.1594/essr2016/P-0013
.
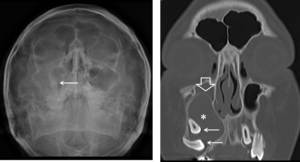
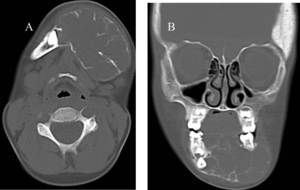
Coronal CT image shows the presence of a cyst in the right maxillary sinus (*). The upper border of the cyst within the right maxillary sinus can be seen (open arrow). 2 teeth can be seen projecting into the cystic lesion (arrows).")
Fig. 1:
Plain radiograph of the face shows opacification of the right maxillary sinus...

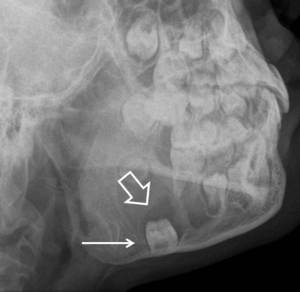
Fig. 2:
Lateral plain radiograph of the mandible shows a large cystic lesion causing...

Fig. 3:
Axial CT image shows the lesion to be cystic and causing bony expansion with...
 in the body of the mandible associated with an unerupted tooth (arrow).")
Fig. 4:
Plain oblique radiograph of the mandible shows the presence of a well-defined...

Fig. 5:
Axial CT image shows similar findings to the plain radiograph

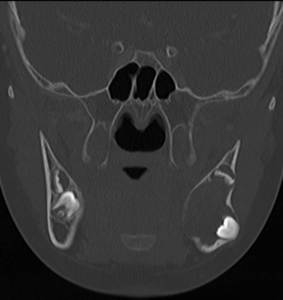
Fig. 6:
Coronal CT image shows similar findings to the plain radiograph
.
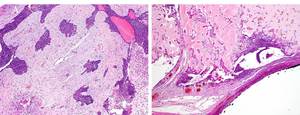
Image courtesy of Dr Derrick Lian, Department of Pathology and Laboratory Medicine, KK Hospital.")
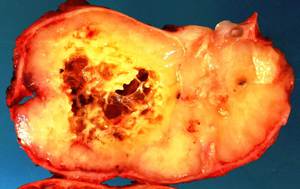
Fig. 7:
Gross specimen of the resected lesion shows a collapsed cyst measuring 2.5 x 2...

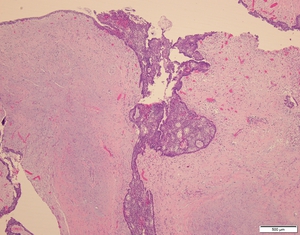
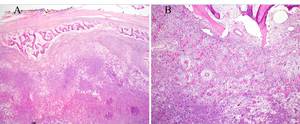
Fig. 8:
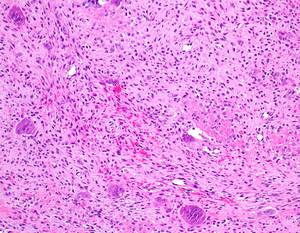
The cyst wall is lined by basaloid epithelium with a plexiform and anastomosing...
Plain radiograph shows a lucent lesion with cortical erosion in the body of the left side of the mandible (arrow). (B and C) Coronal and Axial CT images show the lesion to be slightly higher in attenuation when compared to surrounding soft tissue. Areas of cortical erosion and thinning can be seen indicating that the lesion is aggressive.")
Fig. 9:
(A)Plain radiograph shows a lucent lesion with cortical erosion in the body of...
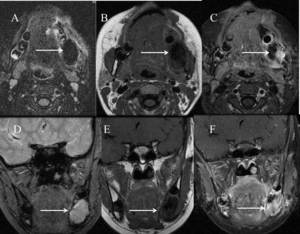
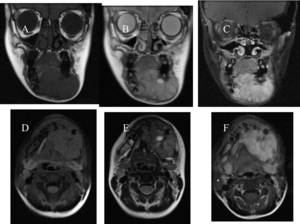
 Axial T2, (B) Axial T1, (C) Axial T1 fat-saturated post contrast, (D) Coronal Gradient echo, (E) Coronal T1 and (F)Coronal T1 fat-saturated post-contrast images shows a lesion of heterogeneous signal intensity in the body of the left side of the mandible showing areas of enhancement post contrast.")
Fig. 10:
(A) Axial T2, (B) Axial T1, (C) Axial T1 fat-saturated post contrast, (D)...

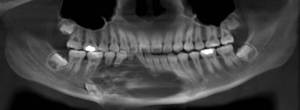
Fig. 12:
Orthopantomogram of the mandible shows a multiloculated lucent lesion just to...
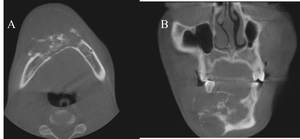
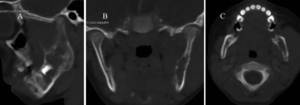
 Axial and (B) Coronal CT images show a destructive, multiloculated lucent lesion in the right side of the body of the mandible.")
Fig. 13:
(A) Axial and (B) Coronal CT images show a destructive, multiloculated lucent...

Fig. 15:
Gross specimen of the resected portion of the mandible shows the lesion...

Fig. 16:
Internal appearance of the lesion shows a cystic part and a solid posterior...
 HE stain of the solid component show islands and nests of epithelial cells with peripheral palisading, within a fibrous stroma. (B) The cyst wall lining shows ameloblastomatous cells with ghost cells.")
Fig. 17:
(A) HE stain of the solid component show islands and nests of epithelial cells...

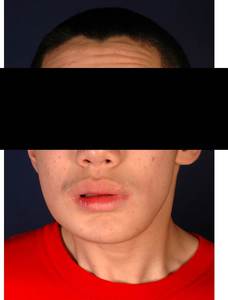
Fig. 11:
Frontal photograph of the patient shows a swelling of the right side of the...

Fig. 14:
3D reconstructed image shows the expansile radiolucent lesion just to the right...

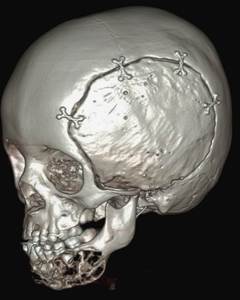
Fig. 18:
Post-operation and reconstruction photograph shows satisfactory result.
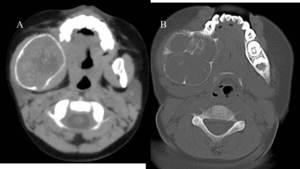
 Axial CT image in soft tissue window and (B) bone window shows the presence of an expansile multiloculated lesion situated in the body of the right side of the mandible.")
Fig. 19:
(A) Axial CT image in soft tissue window and (B) bone window shows the presence...
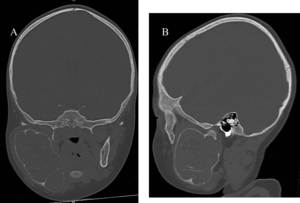
 Coronal and (B) Sagittal CT images show the expansile, multiloculated within the right side of the mandible.")
Fig. 20:
(A) Coronal and (B) Sagittal CT images show the expansile, multiloculated...

Fig. 21:
3D reconstructed CT image shows the multiloculated lesion with bubbly features...

Fig. 22:
Gross photograph of mandibular resection specimen showing a well-circumscribed...
Photomicrograph: H&E-stained photomicrograph (magnification x20) showing thin rim of remnant mandibular cortical bone (top) and subjacent predominantly fibrous tumour with variable cellularity. (B) Photomicrograph: H&E-stained photomicrograph (magnification x100) showing fibrocellular tumour with osteoid and irregular lamellar bone formation. There is no merging of preexisting bony trabeculae (top) with lesional bone.")
Fig. 23:
(A)Photomicrograph: H&E-stained photomicrograph (magnification x20) showing...

Fig. 25:
3D reconstructed CT images shows the multiloculated lesion in the left side of...
 Coronal T1, (B)Coronal T2, (C)Coronal T1 post-contrast, (D)Axial T1 fat-saturated, (E) Axial T2, (F)Axial t1 post-contrast MRI images shows the lesion in the left side of the mandible to be low in signal intensity on T1-weighted imaging, intermediate in signal intensity on T2-weighted imaging and demonstrating contrast enhancement.")
Fig. 26:
(A) Coronal T1, (B)Coronal T2, (C)Coronal T1 post-contrast, (D)Axial T1...

Fig. 27:
The resected specimen is an irregular hard brown piece of tissue measuring 5.5...

Fig. 28:
H&E stained photomicrograph shows a section of bone with a central area...
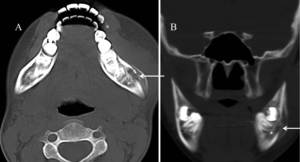
Axial and (B) Coronal CT images show the presence of a multiloculated cystic lesion in the left side of the body of the mandible.")
Fig. 24:
(A)Axial and (B) Coronal CT images show the presence of a multiloculated cystic...
Axial, (B)Coronal (C)3D reconstructed CT images show similar findings to the plain radiograph with better demonstration of the bony expansion and cortical thinning.")
Fig. 30:
(A)Axial, (B)Coronal (C)3D reconstructed CT images show similar findings to the...

Fig. 29:
Plain frontal radiograph shows the presence of bilateral, symmetrical,...

Fig. 31:
The right side of the mandible is larger than the left and the bony matrix has...
Sagittal oblique, (B) Coronal (C) Axial CT images show a lucency with irregular margins involving the left ramus and body of the mandible. Histological diagnosis revealed leukaemic involvement.")
Fig. 32:
Known leukaemic patient with bony infiltration of the left side of the...
Axial (B)Coronal CT images shows a lucent lesion within the left side of the body of the mandible (*) with a cloaca (arrow) and overlying periosteal reaction. Overlying soft tissue swelling is also noted.")
Fig. 33:
(A)Axial (B)Coronal CT images shows a lucent lesion within the left side of the...