ESSR 2016 / P-0020
Heel that hurts
Congress:
ESSR 2016
Poster Number:
P-0020
Type:
Educational Poster
Keywords:
Extremities, Musculoskeletal bone, Musculoskeletal soft tissue, MR, Ultrasound, Plain radiographic studies, Education, Education and training
Authors:
S. B. Gagrani1, S. Lee2, R. Bhatt3; 1Birmingham/UK, 2Leicester/UK, 3Leicester /UK
DOI:
10.1594/essr2016/P-0020

Fig. 1:
Plantar fasciitis: STIR sagittal image showing thickening and hyperintensity of...

Fig. 2:
Plantar fasciitis: STIR coronal image showing marked thickening of central...

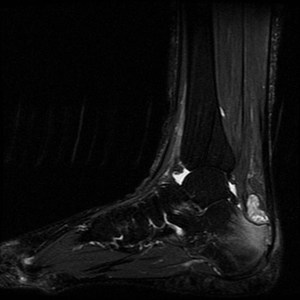
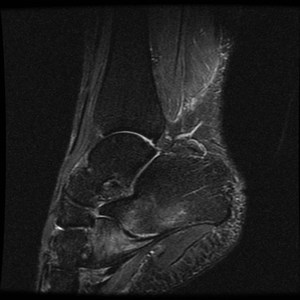
Fig. 3:
Plantar fascia rupture: STIR sagittal image demonstrating almost complete...

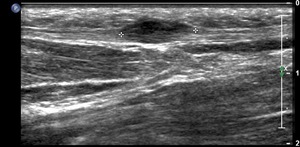
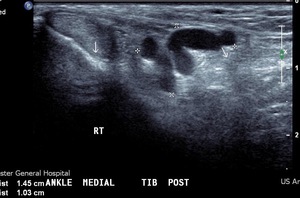
Fig. 4:
Plantar fibroma: Ultrasound image demonstrating a hypoechoic nodular lesion in...

Fig. 5:
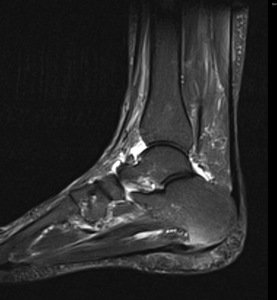
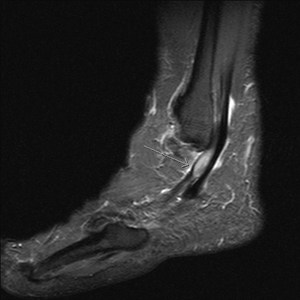
Insertional Achilles tendinitis: T1 sagittal MRI Image shows thickening of the...

Fig. 6:
Insertional Achilles tendinitis: T2 fat suppressed sagittal MRI demonstrates...

Fig. 7:
Insertional Achilles tendinitis with retrocalcaneal bursitis:
Ultrasound image...

Fig. 8:
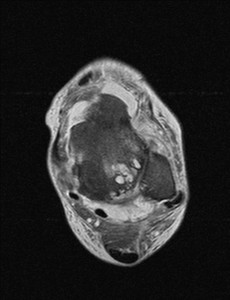
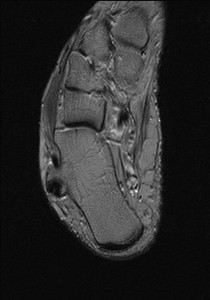
Tenosynovitis of FHL :STIR axial MRI demonstrates fluid in the sheath of flexor...

Fig. 9:
Peroneal tenosynovitis: STIR sagittal MRI image shows thickened hyperintense...

Fig. 10:
Peroneal tendon dislocation: T2 Axial MRI image shows lateral dislocation of...

Fig. 11:
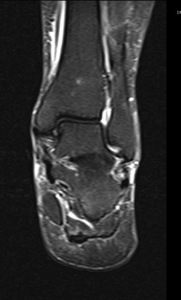
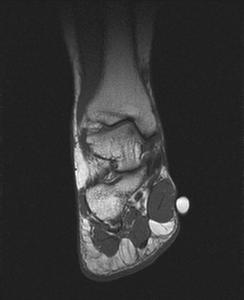
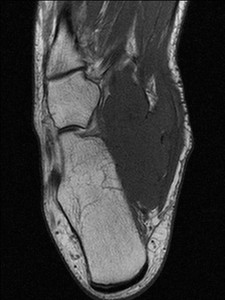
Hypertrophic Abductor hallucis Muscle :T1 coronal image with a skin marker at...

Fig. 12:
Accessory Soleus with a fleshy insertion: Sagittal T1-weighted MR images shows...
 signal intensity in sinus tarsi fat . References: Radiology,NHS Trust, university hospital Leicester-Leicester/UK")
Fig. 14:
Sinus tarsi syndrome: It is a clinical finding that mainly consists of pain...

Fig. 13:
Short Planter ligament sprain:
STIR sagittal image shows the sprain injury of...

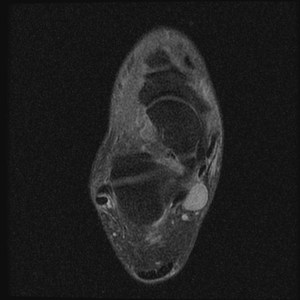
Fig. 15:
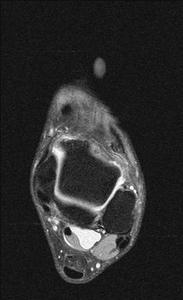
Neurogenic tumour of posterior tibial nerve:STIR axial MRI iamge shows an ovoid...
was caused by plantar calcaneal spur and plantar fasciitis. References: Radiology,NHS Trust, Heartland hospital ,Birmingham uk")
Fig. 16:
Baxter's Neuropathy :In a 53 year old female with heel pain, T1 coronal and...
was caused by planter calcaneal spur and planter fasciitis. References: Radiology,NHS Trust, Heartland hospital Birmingham /UK")
Fig. 17:
Baxter's Neuropathy :In a 53 year old female with heel pain, T1 coronal and...

Fig. 18:
Tarsal coalition: Plain radiograph showing calcaneocuboid coalition.

Fig. 19:
Tarsal coalition : Plain radiograph showing Calcaneonavicular coalition

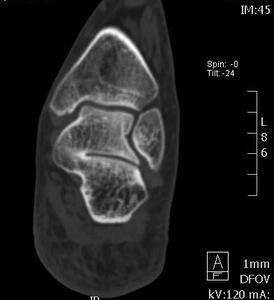
Fig. 20:
Tarsal coalition: Coronal reconstruction of multi-slice CT demostrates osseous...

Fig. 21:
Tarsal coalition: T1 Coronal MRI image showing osseous talocalcaneal coalition.

Fig. 22:
Tarsal coalition: T1 sagittal MRI shows fibrous calcaneonavicular coalition

Fig. 23:
Peroneal tubercle syndrome : T2 axial image shows elongated peroneal tubercle...

Fig. 24:
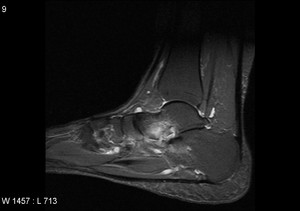
Haglund deformity :T1 and STIR sagittal MRI shows bony prominence is seen on...

Fig. 25:
Haglund deformity :T1 and STIR sagittal MRI shows bony prominence is seen on...
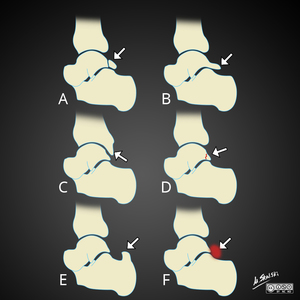
 Os trigonum, B) Stieda syndrome C) Down-sloping posterior tibia D) Fracture through lateral tubercle of posterior process of talus E) Prominent superior calcaneus F) Inflammatory soft tissue. References: Case courtesy of Dr Matt Skalski, Radiopaedia.org, rID: 35398")
Fig. 26:
Different causes of posterior impingement syndrome of ankle.
A) Os trigonum,...

Fig. 27:
Os trigonum : Lateral radiograph of ankle shows large well corticated ossicle...

Fig. 28:
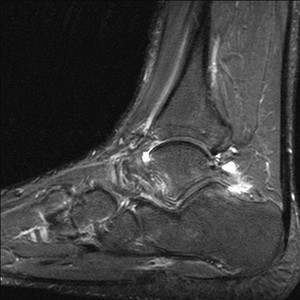
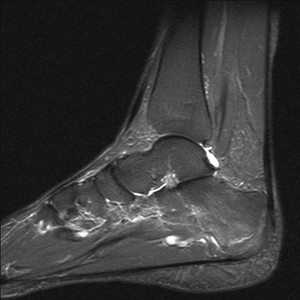
Posterior ankle impingement: Sagittal STIR image of the ankle shows focal fluid...

Fig. 29:
Stress fracture of calcaneum : Plain radiograph showing linear sclerotic line...

Fig. 30:
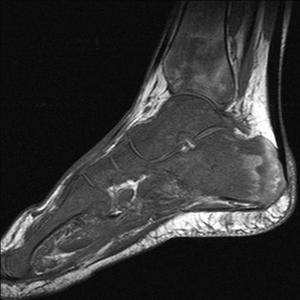
Calcaneal stress fracture: T1 sagittal image demonstrates irregular linear low...

Fig. 31:
Calcaneal Stress fracture: STIR sagittal image demonstrates high signal...

Fig. 32:
Inflammatory arthritis: STIR sagittal image of hind foot shows calcaneo-cuboid...

Fig. 33:
Inflammatory arthritis: STIR sagittal image shows subarticular inflammatory...

Fig. 34:
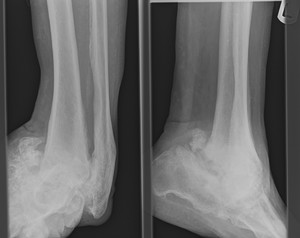
Charcots arthropathy: AP and lateral radiographs of ankle shows marked...

Fig. 35:
Neuropathic arthropathy of mid and hind foot joints: T1 sagittal image of mid...

Fig. 36:
Broadie's abscess: T2 fat suppressed coronal image shows well circumscibed...

Fig. 37:
Lymphoma of foot: T1 and STIR sagittal views show repalcement of bone marrow of...

Fig. 38:
Lymphoma of foot: T1 and STIR sagittal views show repalcement of bone marrow of...

Fig. 39:
Retrocalcaneal buristis

Fig. 40:
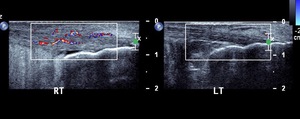
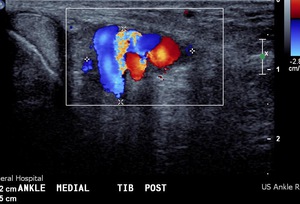
Vascular malformation of tarsal tunnel: Ultrasound with colour doppler imaging...

Fig. 41:
Vascular malformation in tarsal tunnel: Ultrasound with colour doppler imaging...

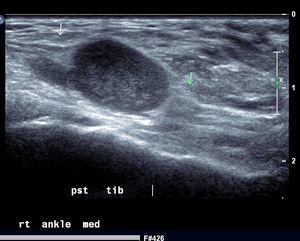
Fig. 42:
Neurogenic tumour of posterior tibial nerve : Ultrasound image of a neurogenic...

Fig. 43:
Tarsal tunnel syndrome due to ganglion cyst: STIR sagittal iamge of hinfoot...

Fig. 44:
Ganglion cyst: STIR sagittal image shows loculated ganglion cyst on lateral...

Fig. 45:
Sarcoma of hinfoot: T1 axial image shows large medium signal intensity soft...